Get your patient on Amphetamine
Amphetamine prescribing information
WARNING: ABUSE, MISUSE, AND ADDICTION
Amphetamine extended-release orally disintegrating tablets have a high potential for abuse and misuse, which can lead to the development of a substance use disorder, including addiction. Misuse and abuse of CNS stimulants, including amphetamine extended-release orally disintegrating tablets, can result in overdose and death [see Overdosage (10) ] , and this risk is increased with higher doses or unapproved methods of administration, such as snorting or injection.
Before prescribing amphetamine extended-release orally disintegrating tablets, assess each patient’s risk for abuse, misuse, and addiction. Educate patients and their families about these risks, proper storage of the drug, and proper disposal of any unused drug. Throughout amphetamine extended-release orally disintegrating tablets treatment, reassess each patient’s risk of abuse, misuse, and addiction and frequently monitor for signs and symptoms of abuse, misuse, and addiction [see Warnings and Precautions (5.1 ), Drug Abuse and Dependence (9.2 )] .
1 INDICATIONS AND USAGE
Amphetamine extended-release orally disintegrating tablets are a central nervous system (CNS) stimulant indicated for the treatment of Attention Deficit Hyperactivity Disorder (ADHD) in patients 6 years and older [see Clinical Studies (14 )] .
Limitations of Use The use of amphetamine extended-release orally disintegrating tablets are not recommended in pediatric patients younger than 6 years of age because they had higher plasma exposure and a higher incidence of adverse reactions (e.g., weight loss) than patients 6 years and older at the same dosage [see Warnings and Precautions (5.5 ), Use in Specific Populations (8.4 )] .
2 DOSAGE AND ADMINISTRATION
2.1 Pre-treatment Screening
Prior to treating patients with amphetamine extended-release orally disintegrating tablets, assess:
- for the presence of cardiac disease (i.e., perform a careful history, family history of sudden death or ventricular arrhythmia, and physical exam) [see Warnings and Precautions (5.2 ) ] .
- the family history and clinically evaluate patients for motor or verbal tics or Tourette’s syndrome before initiating amphetamine extended-release orally disintegrating tablets [see Warnings and Precautions (5.9 )] .
2.2 General Administration Information
Amphetamine extended-release orally disintegrating tablets may be taken orally with or without food. Individualize the dosage according to the therapeutic needs and response of the patient.
Amphetamine extended-release orally disintegrating tablets should be taken as follows:
- The tablet should remain in the blister pack until the patient is ready to take it.
- The patient or caregiver should use dry hands to open the blister.
- Tear along the perforation, bend the blister where indicated and peel back the blister’s labeled backing to take out the tablet. The tablet should not be pushed through the foil.
As soon as the blister is opened, the tablet should be removed and placed on the patient’s tongue.
- The whole tablet should be placed on the tongue and allowed to disintegrate without chewing or crushing.
- The tablet will disintegrate in saliva so that it can be swallowed.
2.3 Dosage Recommendations in Pediatric Patients
The recommended starting dosage is 6.3 mg once daily in the morning. Increase in increments of 3.1 mg or 6.3 mg at weekly intervals. The maximum recommended dose is 18.8 mg daily for patients 6 to 12 years, and 12.5 mg daily for patients 13 to 17 years [see Use in Specific Populations (8.3 ) , Clinical Studies (14 ) ] .
2.4 Dosage Recommendations in Adults
The recommended dose is amphetamine extended-release orally disintegrating tablets 12.5 mg daily.
2.5 Switching from Other Amphetamine Products
Patients taking dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine aspartate monohydrate, and amphetamine sulfate extended-release capsules may be switched to amphetamine extended-release orally disintegrating tablets at the equivalent dose taken once daily [see Clinical Pharmacology (12.3 )] . Refer to Table 1 for equivalent doses of amphetamine extended-release orally disintegrating tablets and dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine aspartate monohydrate, and amphetamine sulfate extended-release capsules. Dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine aspartate monohydrate, and amphetamine sulfate extended-release capsules are also referred to as mixed salts of a single-entity amphetamine product extended-release capsules (MAS ER).
Amphetamine extended-release orally disintegrating tablets | 3.1 mg | 6.3 mg | 9.4 mg | 12.5 mg | 15.7 mg | 18.8 mg |
Dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine aspartate monohydrate, and amphetamine sulfate extended-release capsules Mixed salts of a single-entity amphetamine product extended-release capsules (MAS ER) | 5 mg | 10 mg | 15 mg | 20 mg | 25 mg | 30 mg |
If switching from any other amphetamine products, discontinue that treatment, and titrate with amphetamine extended-release orally disintegrating tablets using the titration schedule [see Dosage and Administration (2.3 ) , (2.4 ) ] .
Do not substitute for other amphetamine products on a milligram-per-milligram basis because of different amphetamine base compositions and differing pharmacokinetic profiles [see Warnings and Precautions (5.9 )] .
2.6 Dosage Modifications Due to Drug Interactions
Agents that alter urinary pH can impact urinary excretion and alter blood levels of amphetamine. Acidifying agents (e.g., ascorbic acid) decrease blood levels, while alkalinizing agents (e.g., sodium bicarbonate) increase blood levels. Adjust amphetamine extended-release orally disintegrating tablets dosage accordingly [see Drug Interactions (7.1 )] .
3 DOSAGE FORMS AND STRENGTHS
Amphetamine extended-release orally disintegrating tablets 3.1 mg are light yellow, mottled round tablets debossed with “A17” on one side and plain on the other side.
Amphetamine extended-release orally disintegrating tablets 6.3 mg are light yellow, mottled round tablets debossed with “A118” on one side and plain on the other side.
Amphetamine extended-release orally disintegrating tablets 9.4 mg are light yellow, mottled round tablets debossed with “A119” on one side and plain on the other side.
Amphetamine extended-release orally disintegrating tablets 12.5 mg are light yellow, mottled round tablets debossed with “A285” on one side and plain on the other side.
Amphetamine extended-release orally disintegrating tablets 15.7 mg are light yellow, mottled round tablets debossed with “A121” on one side and plain on the other side.
Amphetamine extended-release orally disintegrating tablets 18.8 mg are light yellow, mottled round tablets debossed with “A122” on one side and plain on the other side.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Available data from epidemiologic studies and postmarketing reports on the use of amphetamine in pregnant women over decades of use have not identified a drug-associated risk of major birth defects or miscarriage. Neonates exposed to amphetamine in utero are at risk for withdrawal symptoms following delivery. Adverse pregnancy outcomes including premature delivery and low birth weight have been seen in infants born to mothers taking amphetamines during pregnancy (see Clinical Considerations).
No apparent effects on morphological development were observed in embryo-fetal development studies, with oral administration of amphetamine to rats and rabbits during organogenesis. However, in a pre- and post-natal development study, amphetamine (d- to l- ratio of 3:1) administered orally to pregnant rats during gestation and lactation caused a decrease in pup survival and a decrease in pup body weight that correlated with a delay in developmental landmarks at clinically relevant doses of amphetamine. In addition, adverse effects on reproductive performance were observed in pups whose mothers were treated with amphetamine. Long-term neurochemical and behavioral effects have also been reported in animal developmental studies using clinically relevant doses of amphetamine ( see Data ).
The background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Fetal/Neonatal Adverse Reactions
Amphetamines, such as amphetamine extended-release orally disintegrating tablets, cause vasoconstriction and thereby may decrease placental perfusion. In addition, amphetamines can stimulate uterine contractions, increasing the risk of premature delivery. Infants born to mothers taking amphetamines during pregnancy have an increased risk of premature delivery and low birth weight.
Monitor infants born to mothers taking amphetamines for symptoms of withdrawal such as feeding difficulties, irritability, agitation, and excessive drowsiness.
Data
Animal Data
Amphetamine, in the enantiomer ratio present in amphetamine extended-release orally disintegrating tablets, (d- to l-ratio of 3:1), had no apparent effects on embryofetal morphological development or survival when orally administered to pregnant rats and rabbits throughout the period of organogenesis at doses of up to 6 and 16 mg/kg/day, respectively. These doses are approximately 2 and 12 times, respectively, the maximum recommended human dose (MRHD) for adolescents of 12.5 mg/day (as base), on a mg/m 2 body surface area basis. Fetal malformations and death have been reported in mice following parenteral administration of d-amphetamine doses of 50 mg/kg/day (approximately 10 times the MRHD for adolescents on a mg/m 2 basis) or greater to pregnant animals. Administration of these doses was also associated with severe maternal toxicity.
A study was conducted in which pregnant rats received daily oral doses of amphetamine (d- to l-enantiomer ratio of 3:1, the same as in amphetamine extended-release orally disintegrating tablets) of 2, 6, and 10 mg/kg from gestation day 6 to lactation day 20. These doses are approximately 0.8, 2, and 4 times the MRHD for adolescents of 12.5 mg/day (as base), on a mg/m 2 basis. All doses caused hyperactivity and decreased weight gain in the dams. A decrease in pup survival was seen at all doses. A decrease in pup bodyweight was seen at 6 and 10 mg/kg which correlated with delays in developmental landmarks. Increased pup locomotor activity was seen at 10 mg/kg on day 22 postpartum but not at 5 weeks post-weaning. When pups were tested for reproductive performance at maturation, gestational weight gain, number of implantations, and number of delivered pups were decreased in the group whose mothers had been given 10 mg/kg.
A number of studies in rodents indicate that prenatal or early postnatal exposure to amphetamine (d- or d, l-), at doses similar to those used clinically, can result in long-term neurochemical and behavioral alterations. Reported behavioral effects include learning and memory deficits, altered locomotor activity, and changes in sexual function.
8.2 Lactation
Risk Summary
Based on limited case reports in published literature, amphetamine (d- or d, l-) is present in human milk at relative infant doses of 2% to 13.8% of the maternal weight-adjusted dosage and a milk/plasma ratio ranging between 1.9 and 7.5. There are no reports of adverse effects on the breastfed infant. Long-term neurodevelopmental effects on infants from amphetamine exposure are unknown. It is possible that large dosages of amphetamine might interfere with milk production, especially in women whose lactation is not well established. Because of the potential for serious adverse reactions in nursing infants, advise patients that breastfeeding is not recommended during treatment with amphetamine extended-release orally disintegrating tablets.
8.4 Pediatric Use
The safety and effectiveness have been established in pediatric patients with ADHD ages 6 to 17 years of age in three adequate and well-controlled clinical trials of up to 4 weeks in duration [see Adverse Reactions (6.1 ), Clinical Pharmacology (12 ), Clinical Studies (14 )] .
The safety and effectiveness of amphetamine extended-release orally disintegrating tablets have not been established in pediatric patients below the age of 6 years.
In studies evaluating extended-release amphetamine products, patients 4 to <6 years of age had higher systemic amphetamine exposures than those observed in older pediatric patients at the same dosage. Pediatric patients 4 to <6 years of age also had a higher incidence of adverse reactions, including weight loss.
Long-Term Growth Suppression
Growth should be monitored during treatment with stimulants, including amphetamine extended-release orally disintegrating tablets, in pediatric patients aged 6 to 17 years who are not growing or gaining weight as expected may need to have their treatment interrupted [see Warnings and Precautions (5.5 )] .
Juvenile Animal Data
In a juvenile developmental study, rats received daily oral doses of amphetamine (d to l enantiomer ratio of 3:1, the same as in amphetamine extended-release orally disintegrating tablets) of 2, 6, or 20 mg/kg on days 7 to 13 of age; from day 14 to approximately day 60 of age these doses were given twice daily for total daily doses of 4, 12, or 40 mg/kg. The latter doses are approximately 0.6, 2, and 6 times the maximum recommended human dose for children of 18.8 mg/day (as base), on a mg/m 2 basis. Post dosing hyperactivity was seen at all doses; motor activity measured prior to the daily dose was decreased during the dosing period but the decreased motor activity was largely absent after an 18 day drug-free recovery period. Performance in the Morris water maze test for learning and memory was impaired at the 40 mg/kg dose, and sporadically at the lower doses, when measured prior to the daily dose during the treatment period; no recovery was seen after a 19 day drug-free period. A delay in the developmental milestones of vaginal opening and preputial separation was seen at 40 mg/kg but there was no effect on fertility.
8.5 Geriatric Use
Amphetamine extended-release orally disintegrating tablets have not been studied in the geriatric population.
4 CONTRAINDICATIONS
Amphetamine extended-release orally disintegrating tablets are contraindicated:
- In patients known to be hypersensitive to amphetamine, or other components of amphetamine extended-release orally disintegrating tablets. Hypersensitivity reactions such as angioedema and anaphylactic reactions have been reported in patients treated with other amphetamine products [see Adverse Reactions (6.2 )] .
Patients taking monoamine oxidase inhibitors (MAOIs), or within 14 days of stopping MAOIs (including MAOIs such as linezolid or intravenous methylene blue), because of an increased risk of hypertensive crisis [see Warnings and Precautions (5.7 ), Drug Interactions (7.1 )] .
5 WARNINGS AND PRECAUTIONS
5.1 Abuse, Misuse, and Addiction
Amphetamine extended-release orally disintegrating tablets have a high potential for abuse and misuse. The use of amphetamine extended-release orally disintegrating tablets exposes individuals to the risks of abuse and misuse, which can lead to the development of a substance use disorder, including addiction. Amphetamine extended-release orally disintegrating tablets can be diverted for non-medical use into illicit channels or distribution [see Drug Abuse and Dependence (9.2 )] . Misuse and abuse of CNS stimulants, including amphetamine extended-release orally disintegrating tablets, can result in overdose and death [see Overdosage (10 )] , and this risk is increased with higher doses or unapproved methods of administration, such as snorting or injection.
Before prescribing amphetamine extended-release orally disintegrating tablets, assess each patient’s risk for abuse, misuse, and addiction. Educate patients and their families about these risks and proper disposal of any unused drug. Advise patients to store amphetamine extended-release orally disintegrating tablets in a safe place, preferably locked, and instruct patients to not give amphetamine extended-release orally disintegrating tablets to anyone else. Throughout amphetamine extended-release orally disintegrating tablets treatment, reassess each patient’s risk of abuse, misuse, and addiction and frequently monitor for signs and symptoms of abuse, misuse, and addiction.
5.2 Risks to Patients with Serious Cardiac Disease
Sudden death has been reported in patients with structural cardiac abnormalities or other serious cardiac disease who were treated with CNS stimulants at the recommended ADHD dosage.
Avoid amphetamine extended-release orally disintegrating tablets use in patients with known structural cardiac abnormalities, cardiomyopathy, serious cardiac arrhythmia, coronary artery disease, or other serious cardiac disease.
5.3 Increased Blood Pressure and Heart Rate
CNS stimulants cause an increase in blood pressure (mean increase about 2 to 4 mm Hg) and heart rate (mean increase about 3 to 6 bpm). Some patients may have larger increases.
Monitor all amphetamine extended-release orally disintegrating tablets-treated patients for potential tachycardia and hypertension.
5.4 Psychiatric Adverse Reactions
Exacerbation of Pre-existing Psychosis
CNS stimulants may exacerbate symptoms of behavior disturbance and thought disorder in patients with a pre-existing psychotic disorder.
Induction of a Manic Episode in Patients with Bipolar Disorder
CNS stimulants may induce a manic or mixed episode in patients. Prior to initiating amphetamine extended-release orally disintegrating tablets treatment, screen patients for risk factors for developing a manic episode (e.g., comorbid or has a history of depressive symptoms or a family history of suicide, bipolar disorder, and depression).
New Psychotic or Manic Symptoms
CNS stimulants, at the recommended dosage, may cause psychotic or manic symptoms, e.g., hallucinations, delusional thinking, or mania in patients without prior history of psychotic illness or mania. In a pooled analysis of multiple short-term, placebo-controlled studies of CNS stimulants, psychotic or manic symptoms occurred in 0.1% of CNS stimulant-treated patients compared to 0% of placebo-treated patients. If such symptoms occur, consider discontinuing amphetamine extended-release orally disintegrating tablets.
5.5 Long-Term Suppression of Growth in Pediatric Patients
Amphetamine extended-release orally disintegrating tablets are not approved for use and are not recommended in pediatric patients below 6 years of age [see Use in Specific Population (8.4 )] .
CNS stimulants have been associated with weight loss and slowing of growth rate in pediatric patients. Closely monitor growth (weight and height) in amphetamine extended-release orally disintegrating tablets-treated pediatric patients treated with CNS stimulants.
Pediatric patients not growing or gaining height or weight as expected may need to have their treatment interrupted.
5.6 Peripheral Vasculopathy, including Raynaud’s Phenomenon
CNS stimulants, including amphetamine extended-release orally disintegrating tablets, used to treat ADHD are associated with peripheral vasculopathy, including Raynaud’s phenomenon. Signs and symptoms are usually intermittent and mild; however, sequelae have included digital ulceration and/or soft tissue breakdown. Effects of peripheral vasculopathy, including Raynaud’s phenomenon, were observed in postmarketing reports and at the therapeutic dosage of CNS stimulants in all age groups throughout the course of treatment. Signs and symptoms generally improved after dosage reduction or discontinuation of the CNS stimulant.
Careful observation for digital changes is necessary during amphetamine extended-release orally disintegrating tablets-treatment. Further clinical evaluation (e.g., rheumatology referral) may be appropriate for amphetamine extended-release orally disintegrating tablets-treated patients who develop signs or symptoms of peripheral vasculopathy.
5.7 Serotonin Syndrome
Serotonin syndrome, a potentially life-threatening reaction, may occur when amphetamines are used in combination with other drugs that affect the serotonergic neurotransmitter systems such as monoamine oxidase inhibitors (MAOIs), selective serotonin reuptake inhibitors (SSRIs), serotonin norepinephrine reuptake inhibitors (SNRIs), triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, tryptophan, buspirone, and St. John’s Wort [see Drug Interactions (7.1) ] . The coadministration with cytochrome P450 2D6 (CYP2D6) inhibitors may also increase the risk with increased exposure to amphetamine extended-release orally disintegrating tablets. In these situations, consider an alternative non-serotonergic drug or an alternative drug that does not inhibit CYP2D6 [see Drug Interactions (7.1 ) ] .
Serotonin syndrome symptoms may include mental status changes (e.g., agitation, hallucinations, delirium, and coma), autonomic instability (e.g., tachycardia, labile blood pressure, dizziness, diaphoresis, flushing, hyperthermia), neuromuscular symptoms (e.g., tremor, rigidity, myoclonus, hyperreflexia, incoordination), seizures, and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea).
Concomitant use of amphetamine extended-release orally disintegrating tablets with MAOI drugs is contraindicated [see Contraindications (4 )] .
Discontinue treatment with amphetamine extended-release orally disintegrating tablets and any concomitant serotonergic agents immediately if the above symptoms occur, and initiate supportive symptomatic treatment. If concomitant use of amphetamine extended-release orally disintegrating tablets with other serotonergic drugs or CYP2D6 inhibitors is clinically warranted, initiate amphetamine extended-release orally disintegrating tablets with lower doses, monitor patients for the emergence of serotonin syndrome during drug initiation or titration, and inform patients of the increased risk for serotonin syndrome.
5.8 Motor and Verbal Tics, and Worsening of Tourette’s Syndrome
CNS stimulants, including amphetamine, have been associated with the onset or exacerbation of motor and verbal tics. Worsening of Tourette’s syndrome has also been reported [see Adverse Reactions (6.2 )] .
Before initiating amphetamine extended-release orally disintegrating tablets, assess the family history and clinically evaluate patients for tics or Tourette’s syndrome. Regularly monitor amphetamine extended-release orally disintegrating tablets-treated patients for the emergence or worsening of tics or Tourette’s syndrome and discontinue treatment if clinically appropriate.
Potential for Overdose Due to Medication Errors
Medication errors, including substitution and dispensing errors, between amphetamine extended-release orally disintegrating tablets and other amphetamine products could occur, leading to possible overdosage. To avoid substitution errors and overdosage, do not substitute for other amphetamine products on a milligram-per-milligram basis because of different amphetamine base compositions and differing pharmacokinetic profiles [see Dosage and Administration (2.5 )] .
6 ADVERSE REACTIONS
The following adverse reactions are discussed in greater detail in other sections of the labeling:
- Abuse, Misuse, and Addiction [see Boxed Warning, Warnings and Precautions (5.1 ), and Drug Abuse and Dependence (9.2 , 9.3 )]
- Hypersensitivity to amphetamine, or other components of amphetamine extended-release orally disintegrating tablets [see Contraindications (4 )]
- Hypertensive Crisis When Used Concomitantly with Monoamine Oxidase Inhibitors [see Contraindications (4 ) and Drug Interactions (7.1 )]
- Risks to Patients with Serious Cardiac Disease [see Warnings and Precautions (5.2 )]
- Increased Blood Pressure and Heart Rate [see Warnings and Precautions (5.3 )]
- Psychiatric Adverse Reactions [see Warnings and Precautions (5.4 )]
- Long-Term Suppression of Growth in Pediatric Patients [see Warnings and Precautions (5.5 )]
- Peripheral Vasculopathy, including Raynaud’s phenomenon [see Warnings and Precautions (5.6 )]
- Serotonin Syndrome [see Warnings and Precautions (5.7 )]
- Motor and Verbal Tics, and Worsening of Tourette’s Syndrome [see Warnings and Precautions (5.8 )]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The safety of amphetamine extended-release orally disintegrating tablets has been established from adequate and well-controlled studies of single-entity amphetamine product extended-release (MAS ER) capsules [see Clinical Studies (14 )] . The adverse reactions of MAS ER capsules in these adequate and well-controlled studies are described below.
The premarketing development program for MAS ER included exposures in a total of 1,315 participants in clinical trials (635 pediatric patients, 350 adolescent patients, 248 adult patients, and 82 healthy adult subjects). Of these, 635 patients (ages 6 to 12 years) were evaluated in two controlled clinical studies, one open-label clinical study, and two single-dose clinical pharmacology studies (N=40).
Adverse Reactions Leading to Discontinuation of Treatment
The most frequent adverse reactions leading to discontinuation of MAS ER in controlled and uncontrolled, multiple-dose clinical trials of pediatric patients ages 6 to 12 years (N=595) were anorexia (loss of appetite) (2.9%), insomnia (1.5%), weight loss (1.2%), emotional lability (1%), and depression (0.7%).
In a separate placebo-controlled 4-week study in pediatric patients ages 13 to 17 years with ADHD, five patients (2.1%) discontinued treatment due to adverse events among MAS ER-treated patients (N=233) compared to 0% who received placebo (N=54). The most frequent adverse event leading to discontinuation and considered to be drug-related (i.e., leading to discontinuation in at least 1% of MAS ER-treated patients and at a rate at least twice that of placebo) was insomnia (1.3%, n=3).
In one placebo-controlled 4-week study among adults with ADHD with doses 20 mg to 60 mg, 23 patients (12.0%) discontinued treatment due to adverse events among MAS ER-treated patients (N=191) compared to one patient (1.6%) who received placebo (N=64). The most frequent adverse events leading to discontinuation and considered to be drug-related (i.e., leading to discontinuation in at least 1% of MAS ER-treated patients and at a rate at least twice that of placebo) were insomnia (5.2%, n=10), anxiety (2.1%, n=4), nervousness (1.6%, n=3), dry mouth (1.6%, n=3), anorexia (1.6%, n=3), tachycardia (1.6%, n=3), headache (1.6%, n=3), and asthenia (1.0%, n=2).
Adverse Reactions Occurring in Clinical Trials
Adverse reactions reported in a 3-week clinical trial of pediatric patients 6 to 12 years of age and a 4-week clinical trial in pediatric patients 13 to 17 years of age and adults, respectively, treated with MAS ER or placebo are presented in the tables below.
Body System | Adverse Reaction | MAS ER (n=374) | Placebo (n=210) |
General | Abdominal Pain (stomachache) Fever Infection Accidental Injury Asthenia (fatigue) | 14% 5% 4% 3% 2% | 10% 2% 2% 2% 0% |
Digestive System | Loss of Appetite Vomiting Nausea Dyspepsia | 22% 7% 5% 2% | 2% 4% 3% 1% |
Nervous System | Insomnia Emotional Lability Nervousness Dizziness | 17% 9% 6% 2% | 2% 2% 2% 0% |
Metabolic/Nutritional | Weight Loss | 4% | 0% |
Body System | Preferred Term | MAS ER (n=233) | Placebo (n=54) |
General | Abdominal Pain (stomachache) | 11% | 2% |
Digestive System | Loss of Appetite a | 36% | 2% |
Nervous System | Insomnia a | 12% | 4% |
Metabolic/Nutritional | Weight Loss a | 9% | 0% |
• Included doses up to 40 mg | |||
a Dose-related adverse reactions | |||
Note: The following reactions did not meet the criterion for inclusion in Table 3 but were reported by 2% to 4% of adolescent patients receiving MAS ER with a higher incidence than patients receiving placebo in this study: accidental injury, asthenia (fatigue), dry mouth, dyspepsia, emotional lability, nausea, somnolence, and vomiting.
Body System | Preferred Term | MAS ER (n=191) | Placebo ( n=64) |
General | Headache Asthenia | 26% 6% | 13% 5% |
Digestive System | Dry Mouth Loss of Appetite Nausea Diarrhea | 35% 33% 8% 6% | 5% 3% 3% 0% |
Nervous System | Insomnia Agitation Anxiety Dizziness | 27% 8% 8% 7% | 13% 5% 5% 0% |
Cardiovascular System | Tachycardia | 6% | 3% |
Metabolic/Nutritional | Weight Loss | 10% | 0% |
Urogenital System | Urinary Tract Infection | 5% | 0% |
• Included doses up to 60 mg. | |||
Note: The following reactions did not meet the criterion for inclusion in Table 4 but were reported by 2% to 4% of adult patients receiving MAS ER with a higher incidence than patients receiving placebo in this study: infection, photosensitivity reaction, constipation, tooth disorder (e.g., teeth clenching, tooth infection), emotional lability, libido decreased, somnolence, speech disorder (e.g., stuttering, excessive speech), palpitation, twitching, dyspnea, sweating, dysmenorrhea, and impotence.
6.2 Adverse Reactions from Clinical Trials and Spontaneous Postmarketing Reports of Other Amphetamine Products
The following adverse reactions are from clinical trials and spontaneous postmarketing reports of other amphetamine products in pediatric patients and adults with ADHD. Because some of these reactions were reported voluntarily from a population of uncertain size, it is not always possible to estimate their frequency reliably or to establish a causal relationship to drug exposure.
Cardiovascular: Palpitations, sudden death, myocardial infarction. There have been isolated reports of cardiomyopathy associated with chronic amphetamine use.
Central Nervous System: Restlessness, irritability, euphoria, dyskinesia, dysphoria, depression, tremor, aggression, anger, logorrhea, paresthesia (including formication), motor and verbal tics.
Eye Disorders: Vision blurred, mydriasis.
Gastrointestinal: Unpleasant taste, constipation, intestinal ischemia, and other gastrointestinal disturbances.
Allergic: Urticaria, rash, hypersensitivity reactions including angioedema and anaphylaxis. Serious skin rashes, including Stevens-Johnson Syndrome and toxic epidermal necrolysis have been reported.
Endocrine: Impotence, change in libido, frequent or prolonged erections.
Skin: Alopecia.
Musculoskeletal, Connective Tissue, and Bone Disorders: rhabdomyolysis.
Psychiatric Disorders: dermatillomania, bruxism.
Vascular Disorders: Raynaud’s phenomenon.
7 DRUG INTERACTIONS
7.1 Drugs Having Clinically Important Interactions with Amphetamines
MAO Inhibitors (MAOI) | |
Clinical Impact | MAOI antidepressants slow amphetamine metabolism, increasing amphetamines effect on the release of norepinephrine and other monoamines from adrenergic nerve endings causing headaches and other signs of hypertensive crisis. Toxic neurological effects and malignant hyperpyrexia can occur, sometimes with fatal results. |
Intervention | Do not administer amphetamine extended-release orally disintegrating tablets during or within 14 days following the administration of MAOI [see Contraindications (4 )] . |
Serotonergic Drugs | |
Clinical Impact | The concomitant use of amphetamine extended-release orally disintegrating tablets and serotonergic drugs increases the risk of serotonin syndrome. |
Intervention | Initiate with lower doses and monitor patients for signs and symptoms of serotonin syndrome, particularly during amphetamine extended-release orally disintegrating tablets initiation or dosage increase. If serotonin syndrome occurs, discontinue amphetamine extended-release orally disintegrating tablets and the concomitant serotonergic drug(s) [see Warnings and Precautions (5.7 )] . |
| Alkalinizing Agents | |
| Clinical Impact | Increase blood levels and potentiate the action of amphetamine. |
| Intervention | Coadministration of amphetamine extended-release orally disintegrating tablets and gastrointestinal alkalinizing agents should be avoided. |
Acidifying Agents | |
| Clinical Impact | Lower blood levels and efficacy of amphetamines. |
| Intervention | Increase dose based on clinical response. |
| Tricyclic Antidepressants | |
| Clinical Impact | May enhance the activity of tricyclic or sympathomimetic agents causing striking and sustained increases in the concentration of d-amphetamine in the brain; cardiovascular effects can be potentiated. |
| Intervention | Monitor frequently and adjust or use alternative therapy based on clinical response. |
7.2 Drug/Laboratory Test Interactions
Amphetamines can cause a significant elevation in plasma corticosteroid levels. This increase is greatest in the evening. Amphetamines may interfere with urinary steroid determinations.
11 DESCRIPTION
Amphetamine extended-release orally disintegrating tablets contain a 3 to 1 ratio of d- to l-amphetamine, a central nervous system stimulant.
The labeled strengths reflect the amount of amphetamine base in amphetamine extended-release orally disintegrating tablets whereas the strengths of the (mixed salts of a single-entity amphetamine) products are in terms of the amount of amphetamine salts. Table 1 in Section 2.5 details the equivalent amounts of active ingredient in these products.
Structural Formula:
Amphetamine extended-release orally disintegrating tablets is an extended-release orally disintegrating tablet containing 45% immediate-release and 55% delayed-release amphetamine for once daily dosing.
Amphetamine extended-release orally disintegrating tablets also contain the following inactive ingredients: citric acid, colloidal silicon dioxide, crospovidone, fructose, magnesium stearate, mannitol, methacrylic acid and ethyl acrylate copolymer, microcrystalline cellulose, pineapple flavor, sodium polystyrene sulfonate, sucralose, povidone K-30, talc, triethyl citrate and yellow iron oxide.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Amphetamines are non-catecholamine sympathomimetic amines with CNS stimulant activity. The mode of therapeutic action in ADHD is not known. Amphetamines are thought to block the reuptake of norepinephrine and dopamine into the presynaptic neuron and increase the release of these monoamines into the extraneuronal space.
12.3 Pharmacokinetics
Absorption
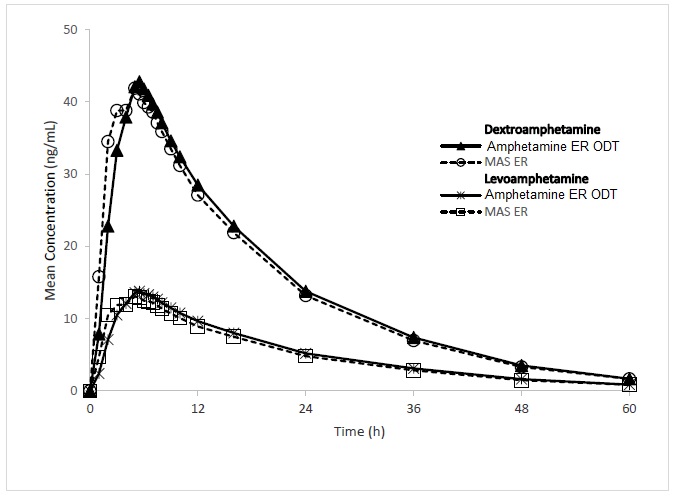
Following a single, 18.8 mg oral dose of amphetamine extended-release orally disintegrating tablets in 40 healthy adult subjects in a crossover study under fasting conditions, d-amphetamine mean (±SD) peak plasma concentrations of 44.9 (±8.9) ng/mL occurred at a median time of 5.0 hours after dosing, and l-amphetamine mean (±SD) peak plasma concentrations of 14.5 (+ 3.0 ng/mL occurred at a median time of 5.25 hours after dosing (Figure 1).
Figure 1: Mean Concentration of D-Amphetamine and L-Amphetamine vs Time for Amphetamine Extended-Release Orally Disintegrating Tablets (18.8 mg) and Mixed Salts of a Single-Entity Amphetamine Product Extended-Release Capsules (MAS ER 30 mg) in the Fasted State
The single dose pharmacokinetics of d-amphetamine under fed conditions are summarized (Table 6) from studies in healthy adults following an oral dose of 18.8 mg amphetamine extended-release orally disintegrating tablets.
PK parameter | Adults Fasted | Adults Fed a |
T max (hr) b | 5.00 (3.00 to 12.00) | 7.00 (3.00 to 16.00) |
T 1/2 (hr) | 11.25±2.0 | 11.33±2.0 |
C max (ng/ml) | 44.9±8.9 | 36.3±6.9 |
AUC inf (hr•ng/mL) | 876.9±182.4 | 856.3±166.1 |
a A high-fat meal was consumed 30 minutes prior to drug administration b Data presented as median (range) | ||
A single dose of amphetamine extended-release orally disintegrating tablets 18.8 mg provided comparable plasma concentration profiles of both d-amphetamine and l-amphetamine to mixed salts of a single-entity amphetamine product extended-release capsules (MAS ER) 30 mg.
The mean elimination half-life for d-amphetamine is 11 hours in adults and 9 to 10 hours in pediatric patients aged 6 to 12 years. For l-amphetamine, the mean elimination half-life in adults is 14 hours and 10 to 11 hours in pediatric patients aged 6 to 12 years. Mean weight-normalized clearance values for d-amphetamine and l-amphetamine decreased slightly with an increase in age.
Food Effect
Food does not affect the extent of absorption of d-amphetamine and l-amphetamine but caused a 19% reduction in C max . Food also prolonged the median t max by approximately 2.0 hours for d-amphetamine and by 2.5 hours for l-amphetamine after administration of amphetamine extended-release orally disintegrating tablets. These changes are not considered clinically significant.
Alcohol Effect
In an in vitro alcohol-induced dose dumping study, a substantial increase in amphetamine release occurred in the presence of 40% alcohol but not with 5%, 10% and 20% alcohol.
Elimination
Metabolism and Excretion
Amphetamine is reported to be oxidized at the 4 position of the benzene ring to form 4-hydroxyamphetamine, or on the side chain α or β carbons to form alpha-hydroxy-amphetamine or norephedrine, respectively. Norephedrine and 4-hydroxy-amphetamine are both active and each is subsequently oxidized to form 4-hydroxy-norephedrine. Alpha-hydroxy-amphetamine undergoes deamination to form phenylacetone, which ultimately forms benzoic acid and its glucuronide and the glycine conjugate hippuric acid. Although the enzymes involved in amphetamine metabolism have not been clearly defined, CYP2D6 is known to be involved with formation of 4-hydroxy-amphetamine. Since CYP2D6 is genetically polymorphic, population variations in amphetamine metabolism are a possibility.
Amphetamine is known to inhibit monoamine oxidase, whereas the ability of amphetamine and its metabolites to inhibit various P450 isozymes and other enzymes has not been adequately elucidated. In vitro experiments with human microsomes indicate minor inhibition of CYP2D6 by amphetamine and minor inhibition of CYP1A2, 2D6, and 3A4 by one or more metabolites. However, due to the probability of auto-inhibition and the lack of information on the concentration of these metabolites relative to in vivo concentrations, no predications regarding the potential for amphetamine or its metabolites to inhibit the metabolism of other drugs by CYP isozymes in vivo can be made.
With normal urine pHs, approximately half of an administered dose of amphetamine is recoverable in urine as derivatives of alpha-hydroxy-amphetamine and approximately another 30% to 40% of the dose is recoverable in urine as amphetamine itself. Since amphetamine has a pKa of 9.9, urinary recovery of amphetamine is highly dependent on pH and urine flow rates. Alkaline urine pHs result in less ionization and reduced renal elimination, and acidic pHs and high flow rates result in increased renal elimination with clearances greater than glomerular filtration rates, indicating the involvement of active secretion. Urinary recovery of amphetamine has been reported to range from 1% to 75%, depending on urinary pH, with the remaining fraction of the dose hepatically metabolized. Consequently, both hepatic and renal dysfunction have the potential to inhibit the elimination of amphetamine and result in prolonged exposures. In addition, drugs that effect urinary pH are known to alter the elimination of amphetamine, and any decrease in amphetamine’s metabolism that might occur due to drug interactions or genetic polymorphisms is more likely to be clinically significant when renal elimination is decreased [see Drug Interactions (7 )] .
Specific Populations
Comparison of the pharmacokinetics of d- and l-amphetamine after oral administration of MAS ER in pediatric patients (6 to 12 years) and adolescent (13 to 17 years) ADHD patients and healthy adult volunteers indicates that body weight is the primary determinant of apparent differences in the pharmacokinetics of d-and l-amphetamine across the age range. Systemic exposure measured by area under the curve to infinity (AUC ∞ ) and maximum plasma concentration (C max ) decreased with increases in body weight, while oral volume of distribution (V Z /F), oral clearance (CL/F), and elimination half-life (t 1/2 ) increased with increases in body weight.
Pediatric Patients
The pharmacokinetics of amphetamine extended-release orally disintegrating tablets in pediatric patients has been established based on the pharmacokinetics of MAS ER in pediatric patients. On a mg/kg weight basis, pediatric patients eliminate amphetamine faster than adults. The elimination half-life (t 1/2 ) is approximately 1 hour shorter for d-amphetamine and 2 hours shorter for l-amphetamine in pediatric patients than in adults. However, for a given dose of MAS ER, pediatric patients had higher systemic exposure to amphetamine (C max and AUC) than adults which was attributed to the higher dose administered to pediatric patients on a mg/kg body weight basis compared to adults. Upon dose normalization on a mg/kg basis, pediatric patients showed 30% less systemic exposure compared to adults.
Gender
Systemic exposure to amphetamine was 20% to 30% higher in women (N=20) than in men (N=20) due to the higher dose administered to women on a mg/kg body weight basis. When the exposure parameters (C max and AUC) were normalized by dose (mg/kg), these differences diminished. Age and gender had no direct effect on the pharmacokinetics of d- and l-amphetamine.
Race
Formal pharmacokinetic studies for race have not been conducted. However, amphetamine pharmacokinetics appeared to be comparable among Caucasians (N=33), Blacks (N=8) and Hispanics (N=10).
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
No evidence of carcinogenicity was found in studies in which d,l-amphetamine (enantiomer ratio of 1:1) was administered to mice and rats in the diet for 2 years at doses of up to 30 mg/kg/day in male mice, 19 mg/kg/day in female mice, and 5 mg/kg/day in male and female rats. These doses are approximately 2.4, 1.5, and 0.8 times, respectively, the maximum recommended human dose for children of 18.8 mg/day (as base), on a mg/m 2 body surface area basis.
Mutagenesis
Amphetamine, in the enantiomer ratio present in amphetamine extended-release orally disintegrating tablets (d- to l-ratio of 3:1), was not clastogenic in the mouse bone marrow micronucleus test in vivo and was negative when tested in the E. coli component of the Ames test in vitro . d,l-Amphetamine (1:1 enantiomer ratio) has been reported to produce a positive response in the mouse bone marrow micronucleus test, an equivocal response in the Ames test, and negative responses in the in vitro sister chromatid exchange and chromosomal aberration assays.
Amphetamine, in the enantiomer ratio present in amphetamine extended-release orally disintegrating tablets (d- to l-ratio of 3:1), did not adversely affect fertility or early embryonic development in the rat at doses of up to 20 mg/kg/day [approximately 8 times the maximum recommended human dose for adolescents of 12.5 mg/day (as base), on a mg/m 2 body surface area basis].
13.2 Animal Toxicology and/or Pharmacology
Acute administration of high doses of amphetamine (d- or d, l-) has been shown to produce long-lasting neurotoxic effects, including irreversible nerve fiber damage, in rodents. The significance of these findings to humans is unknown.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The safety of amphetamine extended-release orally disintegrating tablets has been established from adequate and well-controlled studies of single-entity amphetamine product extended-release (MAS ER) capsules [see Clinical Studies (14 )] . The adverse reactions of MAS ER capsules in these adequate and well-controlled studies are described below.
The premarketing development program for MAS ER included exposures in a total of 1,315 participants in clinical trials (635 pediatric patients, 350 adolescent patients, 248 adult patients, and 82 healthy adult subjects). Of these, 635 patients (ages 6 to 12 years) were evaluated in two controlled clinical studies, one open-label clinical study, and two single-dose clinical pharmacology studies (N=40).
Adverse Reactions Leading to Discontinuation of Treatment
The most frequent adverse reactions leading to discontinuation of MAS ER in controlled and uncontrolled, multiple-dose clinical trials of pediatric patients ages 6 to 12 years (N=595) were anorexia (loss of appetite) (2.9%), insomnia (1.5%), weight loss (1.2%), emotional lability (1%), and depression (0.7%).
In a separate placebo-controlled 4-week study in pediatric patients ages 13 to 17 years with ADHD, five patients (2.1%) discontinued treatment due to adverse events among MAS ER-treated patients (N=233) compared to 0% who received placebo (N=54). The most frequent adverse event leading to discontinuation and considered to be drug-related (i.e., leading to discontinuation in at least 1% of MAS ER-treated patients and at a rate at least twice that of placebo) was insomnia (1.3%, n=3).
In one placebo-controlled 4-week study among adults with ADHD with doses 20 mg to 60 mg, 23 patients (12.0%) discontinued treatment due to adverse events among MAS ER-treated patients (N=191) compared to one patient (1.6%) who received placebo (N=64). The most frequent adverse events leading to discontinuation and considered to be drug-related (i.e., leading to discontinuation in at least 1% of MAS ER-treated patients and at a rate at least twice that of placebo) were insomnia (5.2%, n=10), anxiety (2.1%, n=4), nervousness (1.6%, n=3), dry mouth (1.6%, n=3), anorexia (1.6%, n=3), tachycardia (1.6%, n=3), headache (1.6%, n=3), and asthenia (1.0%, n=2).
Adverse Reactions Occurring in Clinical Trials
Adverse reactions reported in a 3-week clinical trial of pediatric patients 6 to 12 years of age and a 4-week clinical trial in pediatric patients 13 to 17 years of age and adults, respectively, treated with MAS ER or placebo are presented in the tables below.
Body System | Adverse Reaction | MAS ER (n=374) | Placebo (n=210) |
General | Abdominal Pain (stomachache) Fever Infection Accidental Injury Asthenia (fatigue) | 14% 5% 4% 3% 2% | 10% 2% 2% 2% 0% |
Digestive System | Loss of Appetite Vomiting Nausea Dyspepsia | 22% 7% 5% 2% | 2% 4% 3% 1% |
Nervous System | Insomnia Emotional Lability Nervousness Dizziness | 17% 9% 6% 2% | 2% 2% 2% 0% |
Metabolic/Nutritional | Weight Loss | 4% | 0% |
Body System | Preferred Term | MAS ER (n=233) | Placebo (n=54) |
General | Abdominal Pain (stomachache) | 11% | 2% |
Digestive System | Loss of Appetite a | 36% | 2% |
Nervous System | Insomnia a | 12% | 4% |
Metabolic/Nutritional | Weight Loss a | 9% | 0% |
• Included doses up to 40 mg | |||
a Dose-related adverse reactions | |||
Note: The following reactions did not meet the criterion for inclusion in Table 3 but were reported by 2% to 4% of adolescent patients receiving MAS ER with a higher incidence than patients receiving placebo in this study: accidental injury, asthenia (fatigue), dry mouth, dyspepsia, emotional lability, nausea, somnolence, and vomiting.
Body System | Preferred Term | MAS ER (n=191) | Placebo ( n=64) |
General | Headache Asthenia | 26% 6% | 13% 5% |
Digestive System | Dry Mouth Loss of Appetite Nausea Diarrhea | 35% 33% 8% 6% | 5% 3% 3% 0% |
Nervous System | Insomnia Agitation Anxiety Dizziness | 27% 8% 8% 7% | 13% 5% 5% 0% |
Cardiovascular System | Tachycardia | 6% | 3% |
Metabolic/Nutritional | Weight Loss | 10% | 0% |
Urogenital System | Urinary Tract Infection | 5% | 0% |
• Included doses up to 60 mg. | |||
Note: The following reactions did not meet the criterion for inclusion in Table 4 but were reported by 2% to 4% of adult patients receiving MAS ER with a higher incidence than patients receiving placebo in this study: infection, photosensitivity reaction, constipation, tooth disorder (e.g., teeth clenching, tooth infection), emotional lability, libido decreased, somnolence, speech disorder (e.g., stuttering, excessive speech), palpitation, twitching, dyspnea, sweating, dysmenorrhea, and impotence.
16 HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
Amphetamine extended-release orally disintegrating tablets 3.1 mg are light yellow, mottled round tablets debossed with “A17” on one side and plain on the other side and supplied as:
Carton containing 5 blister cards of 6 tablets each, for a total of 30 tablets NDC 0480-3315-65.
Amphetamine extended-release orally disintegrating tablets 6.3 mg are light yellow, mottled round tablets debossed with “A118” on one side and plain on the other side and supplied as:
Carton containing 5 blister cards of 6 tablets each, for a total of 30 tablets NDC 0480-3316-65.
Amphetamine extended-release orally disintegrating tablets 9.4 mg are light yellow, mottled round tablets debossed with “A119” on one side and plain on the other side and supplied as:
Carton containing 5 blister cards of 6 tablets each, for a total of 30 tablets NDC 0480-3317-65.
Amphetamine extended-release orally disintegrating tablets 12.5 mg are light yellow, mottled round tablets debossed with “A285” on one side and plain on the other side and supplied as:
Carton containing 5 blister cards of 6 tablets each, for a total of 30 tablets NDC 0480-3318-65.
Amphetamine extended-release orally disintegrating tablets 15.7 mg are light yellow, mottled round tablets debossed with “A121” on one side and plain on the other side and supplied as:
Carton containing 5 blister cards of 6 tablets each, for a total of 30 tablets NDC 0480-3319-65.
Amphetamine extended-release orally disintegrating tablets 18.8 mg are light yellow, mottled round tablets debossed with “A122” on one side and plain on the other side and supplied as:
Carton containing 5 blister cards of 6 tablets each, for a total of 30 tablets NDC 0480-3320-65.
Storage
Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature].
12.1 Mechanism of Action
Amphetamines are non-catecholamine sympathomimetic amines with CNS stimulant activity. The mode of therapeutic action in ADHD is not known. Amphetamines are thought to block the reuptake of norepinephrine and dopamine into the presynaptic neuron and increase the release of these monoamines into the extraneuronal space.