Get your patient on Arestin - Minocycline Hydrochloride powder (Minocycline Hydrochloride)
Arestin - Minocycline Hydrochloride powder prescribing information
INDICATIONS AND USE
ARESTIN is indicated as an adjunct to scaling and root planing procedures for reduction of pocket depth in patients with adult periodontitis. ARESTIN may be used as part of a periodontal maintenance program which includes good oral hygiene and scaling and root planing.
DOSAGE AND ADMINISTRATION
ARESTIN is provided as a dry powder, packaged in a unit-dose cartridge with a deformable tip (see Figure 1), which is inserted into a spring-loaded cartridge handle mechanism (see Figure 2) to administer the product.
The oral health care professional removes the disposable cartridge from its pouch and connects the cartridge to the handle mechanism (see Figures 3-4 ). ARESTIN is a variable dose product, dependent on the size, shape, and number of pockets being treated. In US clinical trials, up to 122 unit-dose cartridges were used in a single visit and up to 3 treatments, at 3-month intervals, were administered in pockets with pocket depth of 5 mm or greater.
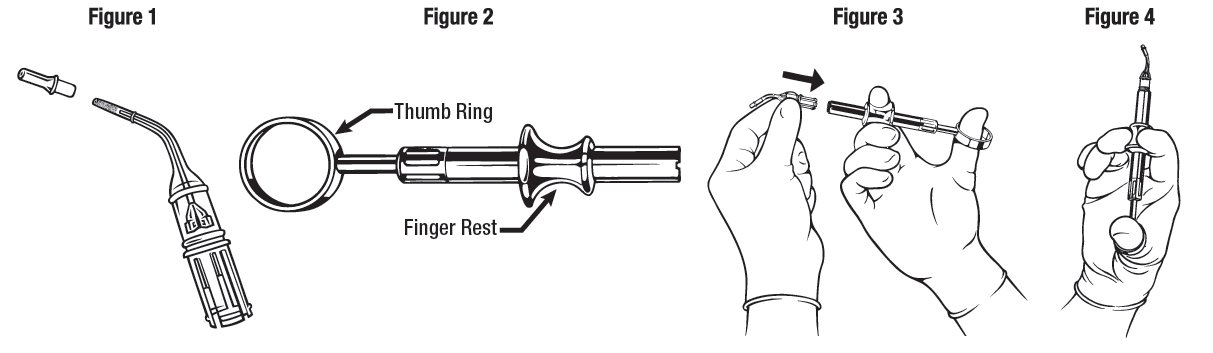
The administration of ARESTIN does not require local anesthesia. Professional subgingival administration is accomplished by inserting the unit-dose cartridge to the base of the periodontal pocket and then pressing the thumb ring in the handle mechanism to expel the powder while gradually withdrawing the tip from the base of the pocket. The handle mechanism should be sterilized between patients. ARESTIN does not have to be removed, as it is bioresorbable, nor is an adhesive or dressing required.
CONTRAINDICATIONS
ARESTIN should not be used in any patient who has a known sensitivity to minocycline or tetracyclines.
ADVERSE REACTIONS
The most frequently reported non-dental, treatment-emergent adverse events in the 3 multicenter US trials were headache, infection, flu syndrome, and pain.
| SRP Alone N=250 | SRP + Vehicle N=249 | SRP + ARESTIN ® N=423 | |
|---|---|---|---|
Number (%) of Subjects Treatment-emergent AEs | 62.4% | 71.9% | 68.1% |
Total Number of AEs | 543 | 589 | 987 |
Periodontitis | 25.6% | 28.1% | 16.3% |
Tooth Disorder | 12.0% | 13.7% | 12.3% |
Tooth Caries | 9.2% | 11.2% | 9.9% |
Dental Pain | 8.8% | 8.8% | 9.9% |
Gingivitis | 7.2% | 8.8% | 9.2% |
Headache | 7.2% | 11.6% | 9.0% |
Infection | 8.0% | 9.6% | 7.6% |
Stomatitis | 8.4% | 6.8% | 6.4% |
Mouth Ulceration | 1.6% | 3.2% | 5.0% |
Flu Syndrome | 3.2% | 6.4% | 5.0% |
Pharyngitis | 3.2% | 1.6% | 4.3% |
Pain | 4.0% | 1.2% | 4.3% |
Dyspepsia | 2.0% | 0 | 4.0% |
Infection Dental | 4.0% | 3.6% | 3.8% |
Mucous Membrane Disorder | 2.4% | 0.8% | 3.3% |
The change in clinical attachment levels was similar across all study arms, suggesting that neither the vehicle nor ARESTIN compromise clinical attachment.
Postmarketing Experience
The following adverse reaction has been identified during postapproval use of minocycline products when taken orally. Because this reaction is reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Skin and subcutaneous tissue disorders: Acute febrile neutrophilic dermatosis (Sweet’s syndrome).
To report SUSPECTED ADVERSE REACTIONS, contact OraPharma at 1-800-321-4576 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DESCRIPTION
ARESTIN (minocycline hydrochloride) microspheres, 1 mg is a subgingival sustained-release product containing the antibiotic minocycline hydrochloride incorporated into a bioresorbable polymer, Poly (glycolide-co-dl-lactide) or PGLA, for professional subgingival administration into periodontal pockets. Each unit-dose cartridge delivers minocycline hydrochloride equivalent to 1 mg of minocycline free base.
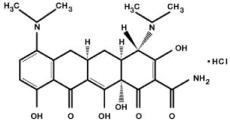
The molecular formula of minocycline hydrochloride is C 23 H 27 N 3 O 7 ● HCl, and the molecular weight is 493.94. The structural formula of minocycline hydrochloride is:
CLINICAL PHARMACOLOGY
Mechanism of Action
The mechanism of action of ARESTIN as an adjunct to scaling and root planing procedures for reduction of pocket depth in patients with adult periodontitis is unknown.
Microbiology
Minocycline, a member of the tetracycline class of antibiotics, has a broad spectrum of activity. It is bacteriostatic and exerts its antimicrobial activity by inhibiting protein synthesis. In vitro susceptibility testing has shown that the organisms Porphyromonas gingivalis, Prevotella intermedia, Fusobacterium nucleatum, Eikenella corrodens , and Actinobacillus actinomycetemcomitans , which are associated with periodontal disease, are susceptible to minocycline at concentrations of ≤8 mcg/mL; qualitative and quantitative changes in plaque microorganisms have not been demonstrated in subjects with periodontitis, using this product.
The emergence of minocycline-resistant bacteria in single-site plaque samples was studied in subjects before and after treatment with ARESTIN at 2 centers. There was a slight increase in the numbers of minocycline-resistant bacteria at the end of the 9-month study period; however, the number of subjects studied was small and the clinical significance of these findings is unknown.
The emergence of minocycline-resistant bacteria and changes in the presence of Candida albicans and Staphylococcus aureus in the gastrointestinal tract were studied in subjects treated with ARESTIN in one phase 3 study. No changes in the presence of minocycline-resistant bacteria or Candida albicans or Staphylococcus aureus were seen at the end of the 56-day study period.
Pharmacokinetics
In a pharmacokinetic study, 18 subjects (10 men and 8 women) with moderate to advanced chronic periodontitis were treated with a mean dose of 46.2 mg (25 to 112 unit doses) of ARESTIN. After fasting for at least 10 hours, subjects received subgingival application of ARESTIN (1 mg per treatment site) following scaling and root planing at a minimum of 30 sites on at least 8 teeth. Investigational drug was administered to all eligible sites ≥5 mm in probing depth. Mean dose normalized saliva AUC and C max were found to be approximately 125 and 1000 times higher than those of serum parameters, respectively.
Clinical Studies
In 2 well-controlled, multicenter, investigator-blind, vehicle-controlled, parallel-design studies (3 arms), 748 subjects (study OPI-103A=368, study OPI-103B=380) with generalized moderate to advanced adult periodontitis characterized by a mean probing depth of 5.90 and 5.81 mm, respectively, were enrolled. Subjects received 1 of 3 treatments: (1) scaling and root planing (SRP), (2) SRP + vehicle (bioresorbable polymer, PGLA), and (3) SRP + ARESTIN. To qualify for the study, subjects were required to have 4 teeth with periodontal pockets of 6 to 9 mm that bled on probing. However, treatment was administered to all sites with mean probing depths of 5 mm or greater. Subjects studied were in good general health. Subjects with poor glycemic control or active infectious diseases were excluded from the studies. Retreatment occurred at 3 and 6 months after initial treatment, and any new site with pocket depth ≥5 mm also received treatment. Subjects treated with ARESTIN were found to have statistically significantly reduced probing pocket depth compared with those treated with SRP alone or SRP + vehicle at 9 months after initial treatment, as shown in Table 1 .
| Time | Study OPI-103A N=368 | Study OPI-103B N=380 | ||||
|---|---|---|---|---|---|---|
| SRP Alone n=124 | SRP + Vehicle n=123 | SRP + ARESTIN n=121 | SRP Alone n=126 | SRP + Vehicle n=126 | SRP + ARESTIN n=128 | |
| SE = standard error; SRP = scaling and root planing; PD = pocket depth | ||||||
| Significantly different from SRP: •(P ≤0.05); ••(P ≤0.001) | ||||||
| Significantly different from SRP + vehicle: †† (P ≤0.001) | ||||||
PD (mm) at Baseline [Mean ± SE] | 5.88 | 5.91 | 5.88 | 5.79 | 5.82 | 5.81 |
±0.04 | ±0.04 | ±0.04 | ±0.03 | ±0.04 | ±0.04 | |
PD (mm) Change from Baseline at 9 Months [Mean ± SE] | -1.04 | -0.90 | -1.20• †† | -1.32 | -1.30 | -1.63•• †† |
±0.07 | ±0.54 | ±0.07 | ±0.07 | ±0.07 | ±0.07 | |
In these 2 studies, an average of 29.5 (5-114), 31.7 (4-137), and 31 (5-108) sites were treated at baseline in the SRP alone, SRP + vehicle, and SRP + ARESTIN groups, respectively. When these studies are combined, the mean pocket depth change at 9 months was -1.18 mm, -1.10 mm, and -1.42 mm for SRP alone, SRP + vehicle, and SRP + ARESTIN, respectively.
Table 2: Numbers (Percentage) of Pockets Showing a Change of Pocket Depth ≥2 mm at
| Study OPI-103A | Study OPI-103B | |||||
|---|---|---|---|---|---|---|
| SRP Alone | SRP + Vehicle | SRP + ARESTIN | SRP Alone | SRP + Vehicle | SRP + ARESTIN | |
Pockets | 1046 | 927 | 1326 | 1692 | 1710 | 2082 |
≥2 mm (% of Total) | (31.1%) | (25.7%) | (36.5%) | (42.2%) | (40.0%) | (51.0%) |
Pockets | 417 | 315 | 548 | 553 | 524 | 704 |
≥3 mm (% of Total) | (12.4%) | (8.7%) | (15.1%) | (13.8%) | (12.3%) | (17.3%) |
SRP + ARESTIN resulted in a greater percentage of pockets showing a change of PD ≥2 mm and ≥3 mm compared to SRP alone at 9 months, as shown in Table 2 .
| SRP Alone | SRP + Vehicle | SRP + ARESTIN | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SRP = scaling and root planing; YOA = years of age; CV = cardiovascular | |||||||||||||||||
Smokers | n=91 -0.96 (±0.09) mm | n=90 -0.98 (±0.07) mm | n=90 -1.24 (±0.09) mm•• | ||||||||||||||
Nonsmokers | n=159 -1.31 (±0.06) mm | n=159 -1.17 (±0.07) mm | n=159 -1.53 (±0.06) mm•• | ||||||||||||||
Subjects >50 YOA | n=21 -1.07 (±0.09) mm | n=81 -0.92 (±0.08) mm | n=107 -1.42 (±0.08) mm•• | ||||||||||||||
Subjects ≤50 YOA | n=167 -1.24 (±0.06) mm | n=168 -1.19 (±0.06) mm | n=142 -1.43 (±0.07) mm• | ||||||||||||||
Subjects with CV Disease | n=36 -0.99 (±0.13) mm | n=29 -1.06 (±0.14) mm | n=36 -1.56 (±0.14) mm•• | ||||||||||||||
Subjects without CV Disease | n=214 -1.22 (±0.06) mm | n=220 -1.11 (±0.05) mm | n=213 -1.40 (±0.06) mm•• | ||||||||||||||
•SRP vs SRP + ARESTIN P ≤0.05; ••SRP vs SRP + ARESTIN P ≤ 0.001
In both studies, the following patient subgroups were prospectively analyzed: smokers, subjects over and under 50 years of age, and subjects with a previous history of cardiovascular disease. The results of the combined studies are presented in Table 3 .
In smokers, the mean reduction in pocket depth at 9 months was less in all treatment groups than in nonsmokers, but the reduction in mean pocket depth at 9 months with SRP + ARESTIN was significantly greater than with SRP + vehicle or SRP alone.
Table 4: Mean Pocket Depth Change in Subjects with Mean Baseline
| Study OPI-103A | Study OPI-103B | |||||
|---|---|---|---|---|---|---|
| Mean Baseline Pocket Depth | SRP Alone | SRP + Vehicle | SRP + ARESTIN | SRP Alone | SRP + Vehicle | SRP + ARESTIN |
≥5 mm (n) | -1.04 mm (124) | -0.90 mm (123) | -1.20 mm• (121) | -1.32 mm (126) | -1.30 mm (126) | -1.63 mm• (128) |
≥6 mm (n) | -0.91 mm (34) | -0.77 mm (46) | -1.40 mm• (45) | -1.33 mm (37) | -1.46 mm (40) | -1.69 mm• (25) |
≥7 mm (n) | -1.10 mm (4) | -0.46 mm (5) | -1.91 mm (3) | -1.72 mm (3) | -1.11 mm (3) | -2.84 mm (2) |
•Statistically significant comparison between SRP + ARESTIN and SRP alone
The combined data from these 2 studies also show that for pockets 5 mm to 7 mm at baseline, greater reductions in pocket depth occurred in pockets that were deeper at baseline.
HOW SUPPLIED
ARESTIN ® (minocycline hydrochloride) microspheres, 1 mg is supplied as follows:
NDC 65976-100-01 1 unit-dose cartridge with desiccant in a heat-sealed, foil-laminated pouch
NDC 65976-100-24 12 unit-dose cartridges in 1 tray with desiccant in a heat-sealed, foil-laminated, resealable pouch. There are 2 pouches in each box.
Each unit-dose cartridge contains the product identifier “OP-1.”
Storage Conditions
Store at 20° to 25°C (68° to 77°F)/60% RH: excursions permitted to 15° to 30°C (59° to 86°F). Avoid exposure to excessive heat.
Mechanism of Action
The mechanism of action of ARESTIN as an adjunct to scaling and root planing procedures for reduction of pocket depth in patients with adult periodontitis is unknown.