Get your patient on Clindamycin Phosphate 1.2% And Tretinoin 0.025%- Clindamycin Phosphate And Tretinoin gel (Clindamycin Phosphate And Tretinoin)
Clindamycin Phosphate 1.2% And Tretinoin 0.025%- Clindamycin Phosphate And Tretinoin gel prescribing information
INDICATIONS AND USAGE
Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel is indicated for the topical treatment of acne vulgaris in patients 12 years or older.
DOSAGE AND ADMINISTRATION
At bedtime, squeeze a pea-sized amount of medication onto one fingertip, dot onto the chin, cheeks, nose, and forehead, then gently rub over the entire face. Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel should be kept away from the eyes, the mouth, angles of the nose, and mucous membranes.
Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel is not for oral, ophthalmic, or intravaginal use.
DOSAGE FORMS AND STRENGTHS
Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel, a combination of a lincosamide antibiotic and a retinoid, contains clindamycin phosphate 1.2% and tretinoin 0.025%, formulated as a topical gel. Each gram of Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel contains, as dispensed, 10 mg (1%) clindamycin as phosphate, and 0.25 mg (0.025%) tretinoin in an aqueous-based gel. Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel is available in 30 gram and 60 gram tubes.
USE IN SPECIFIC POPULATIONS
Pregnancy
Pregnancy Category C. There are no well-controlled trials in pregnant women treated with Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel. Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel was tested for maternal and developmental toxicity in New Zealand White Rabbits with topical doses of 60, 180 and 600 mg/kg/day. Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel at 600 mg/kg/day (approximately 12 times the recommended clinical dose assuming 100% absorption and based on body surface area comparison) was considered to be the no-observed-adverse-effect level (NOAEL) for maternal and developmental toxicity following dermal administration of Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel for 2 weeks prior to artificial insemination and continuing until gestation day 18, inclusive. For purposes of comparisons of the animal exposure to human exposure, the recommended clinical dose is defined as 1 g of Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel applied daily to a 60 kg person.
Clindamycin
Teratology (Segment II) studies using clindamycin were performed orally in rats (up to 600 mg/kg/day) and mice (up to 100 mg/kg/day) (583 and 49 times amount of clindamycin in the recommended clinical dose based on body surface area comparison, respectively) or with subcutaneous doses of clindamycin up to 180 mg/kg/day (175 and 88 times the amount of clindamycin in the recommended clinical dose based on body surface area comparison, respectively) revealed no evidence of teratogenicity.
Tretinoin
In oral Segment III studies in rats with tretinoin, decreased survival of neonates and growth retardation were observed at doses in excess of 2 mg/kg/day (~78 times the recommended clinical dose assuming 100% absorption and based on body surface area comparison).
With widespread use of any drug, a small number of birth defect reports associated temporally with the administration of the drug would be expected by chance alone. Thirty cases of temporally associated congenital malformations have been reported during two decades of clinical use of another formulation of topical tretinoin. Although no definite pattern of teratogenicity and no causal association have been established from these cases, five of the reports describe the rare birth defect category, holoprosencephaly (defects associated with incomplete midline development of the forebrain). The significance of these spontaneous reports in terms of risk to the fetus is not known.
Dermal tretinoin has been shown to be fetotoxic in rabbits when administered in doses 40 times the recommended human clinical dose based on body surface area comparison. Oral tretinoin has been shown to be fetotoxic in rats when administered in doses 78 times the recommended clinical dose based on body surface area comparison.
Nursing Mothers
It is not known whether clindamycin is excreted in human milk following use of Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel. However, orally and parenterally administered clindamycin has been reported to appear in breast milk. Because of the potential for serious adverse reactions in nursing infants, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother. It is not known whether tretinoin is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel is administered to a nursing woman.
Pediatric Use
Safety and effectiveness of Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel in pediatric patients under the age of 12 have not been established.
Clinical trials of Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel included patients 12-17 years of age. [See Clinical Studies (14) .]
Geriatric Use
Clinical studies of Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects.
CONTRAINDICATIONS
Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel is contraindicated in patients with regional enteritis, ulcerative colitis, or history of antibiotic-associated colitis.
WARNINGS AND PRECAUTIONS
- Colitis: Clindamycin can cause severe colitis, which may result in death. Diarrhea, bloody diarrhea, and colitis (including pseudomembranous colitis) have been reported with the use of clindamycin. Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel should be discontinued if significant diarrhea occurs. (5.1 )
- Ultraviolet Light and Environmental Exposures: Avoid exposure to sunlight and sunlamps. Wear sunscreen daily. (5.2 )
Colitis
Systemic absorption of clindamycin has been demonstrated following topical use of this product. Diarrhea, bloody diarrhea, and colitis (including pseudomembranous colitis) have been reported with the use of topical clindamycin. When significant diarrhea occurs, Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel should be discontinued.
Severe colitis has occurred following oral or parenteral administration of clindamycin with an onset of up to several weeks following cessation of therapy. Antiperistaltic agents such as opiates and diphenoxylate with atropine may prolong and/or worsen severe colitis. Severe colitis may result in death.
Studies indicate a toxin(s) produced by clostridia is one primary cause of antibiotic-associated colitis. The colitis is usually characterized by severe persistent diarrhea and severe abdominal cramps and may be associated with the passage of blood and mucus. Stool cultures for Clostridium difficile and stool assay for C. difficile toxin may be helpful diagnostically.
Ultraviolet Light and Environmental Exposure
Exposure to sunlight, including sunlamps, should be avoided during the use of Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel, and patients with sunburn should be advised not to use the product until fully recovered because of heightened susceptibility to sunlight as a result of the use of tretinoin. Patients who may be required to have considerable sun exposure due to occupation and those with inherent sensitivity to the sun should exercise particular caution. Daily use of sunscreen products and protective apparel (e.g., a hat) are recommended. Weather extremes, such as wind or cold, also may be irritating to patients under treatment with Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel.
ADVERSE REACTIONS
Observed local adverse reactions in patients treated with Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel were skin erythema, scaling, itching, burning, and stinging. Other most commonly reported adverse events (≥1% in patients treated with Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel) were nasopharyngitis, pharyngolaryngeal pain, dry skin, cough, and sinusitis. (6.1 )
To report SUSPECTED ADVERSE REACTIONS, contact Oceanside Pharmaceuticals at 1-800-321-4576 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Clinical Studies Experience
Because clinical trials are conducted under prescribed conditions, adverse reaction rates observed in the clinical trial may not reflect the rates observed in practice. The adverse reaction information from clinical trials does, however, provide a basis for identifying the adverse reactions that appear to be related to drug use for approximating rates.
The safety data presented in Table 1 (below) reflects exposure to Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel in 1853 patients with acne vulgaris. Patients were 12 years and older and were treated once daily for 12 weeks. Adverse reactions that were reported in ≥1% of patients treated with Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel were compared to adverse reactions in patients treated with clindamycin phosphate 1.2% in vehicle gel, tretinoin 0.025% in vehicle gel, and the vehicle gel alone:
| Clindamycin Phosphate 1.2% and Tretinoin 0.025%Gel N=1853 N (%) | Clindamycin N=1428 N (%) | Tretinoin N=846 N (%) | Vehicle N=423 N (%) | |
|---|---|---|---|---|
PATIENTS WITH AT LEAST ONE AR | 497 (27) | 342 (24) | 225 (27) | 91 (22) |
Nasopharyngitis | 65 (4) | 64 (5) | 16 (2) | 5 (1) |
Pharyngolaryngeal pain | 29 (2) | 18 (1) | 5 (1) | 7 (2) |
Dry skin | 23 (1) | 7 (1) | 3 (<1) | 0 (0) |
Cough | 19 (1) | 21 (2) | 9 (1) | 2 (1) |
Sinusitis | 19 (1) | 19 (1) | 15 (2) | 4 (1) |
NOTE: Formulations used in all treatment arms were in the Clindamycin Phosphate 1.2% and Tretinoin 0.025% vehicle gel. | ||||
Cutaneous safety and tolerance evaluations were conducted at each study visit in all of the clinical trials by assessment of erythema, scaling, itching, burning, and stinging:
| Local Reaction | Baseline N=1835 N (%) | End of Treatment N=1614 N (%) |
|---|---|---|
Erythema | 636 (35) | 416 (26) |
Scaling | 237 (13) | 280 (17) |
Itching | 189 (10) | 70 (4) |
Burning | 38 (2) | 56 (4) |
Stinging | 33 (2) | 27 (2) |
At each study visit, application site reactions on a scale of 0 (none), 1 (mild), 2 (moderate), and 3 (severe), and the mean scores were calculated for each of the local skin reactions. In Studies 1 and 2, 1277 subjects enrolled with moderate to severe acne, 854 subjects treated with Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel and 423 treated with vehicle. Analysis over the 12-week period demonstrated that cutaneous irritation scores for erythema, scaling, itching, burning, and stinging peaked at 2 weeks of therapy, and were slightly higher for the Clindamycin Phosphate 1.2% and Tretinoin 0.025%-treated group, decreasing thereafter.
One open-label 12-month safety study for Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel showed a similar adverse reaction profile as seen in the 12-week studies. Eighteen out of 442 subjects (4%) reported gastrointestinal symptoms.
DRUG INTERACTIONS
Concomitant Topical Medication
Concomitant topical medication, medicated or abrasive soaps and cleansers, soaps and cosmetics that have a strong drying effect, and products with high concentrations of alcohol, astringents, spices or lime should be used with caution. When used with Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel, there may be increased skin irritation.
Erythromycin
Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel should not be used in combination with erythromycin-containing products due to its clindamycin component. In vitro studies have shown antagonism between these two antimicrobials. The clinical significance of this in vitro antagonism is not known.
Neuromuscular Blocking Agents
Clindamycin has been shown to have neuromuscular blocking properties that may enhance the action of other neuromuscular blocking agents. Therefore, Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel should be used with caution in patients receiving such agents.
DESCRIPTION
Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel is an antibiotic and retinoid combination gel product with two active ingredients. Clindamycin phosphate is a water-soluble ester of the semi-synthetic antibiotic produced by a 7(S)-chloro-substitution of the 7(R)-hydroxyl group of the parent antibiotic lincomycin.
The chemical name for clindamycin phosphate is Methyl 7-chloro-6,7,8-trideoxy-6-(1-methyl- trans -4-propyl-L-2-pyrrolidinecarboxamido)-1-thio-L- threo -α-D- galacto -octopyranoside 2-(dihydrogen phosphate). The structural formula for clindamycin phosphate is represented below:
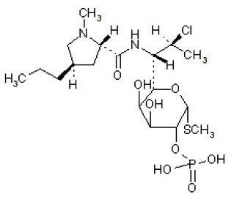
Clindamycin phosphate: Molecular Formula: C 18 H 34 ClN 2 O 8 PS Molecular Weight: 504.97
The chemical name for tretinoin is 3,7-Dimethyl-9-(2,6,6-trimethyl-1-cyclohexen-1-yl)-2,4,6,8 nonatetraenoic acid (all- trans form). The structural formula for tretinoin is represented below:
Tretinoin:
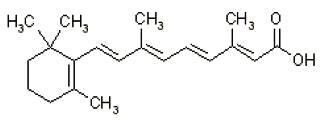
Molecular Formula: C 20 H 28 O 2 Molecular Weight: 300.44
Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel contains the following inactive ingredients: butylated hydroxytoluene NF, carbomer 981 NF, citric acid USP, edetate disodium USP, glycerin USP, methylparaben NF, polysorbate 80 NF, propylparaben NF, purified water USP and tromethamine USP.
CLINICAL PHARMACOLOGY
Mechanism of Action
Clindamycin
[See Microbiology (12.4) .]
Tretinoin
Although the exact mode of action of tretinoin is unknown, current evidence suggests that topical tretinoin decreases cohesiveness of follicular epithelial cells with decreased microcomedo formation.
Additionally, tretinoin stimulates mitotic activity and increased turnover of follicular epithelial cells causing extrusion of the comedones.
Pharmacokinetics
In an open-label, multiple-dose study treating 12 subjects with moderate to severe acne, the percutaneous absorption of tretinoin following 14 consecutive daily applications of approximately 4 g of Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel was minimal. Quantifiable tretinoin plasma concentrations ranged from 1.0 to 1.6 ng/mL, with unquantifiable plasma concentrations in 50% to 92% of subjects at any given timepoint following administration. The plasma concentrations of the key tretinoin metabolites, 13-cis-retinoic acid and 4-oxo-13-cis-retinoic acid, ranged from 1.0 to 1.4 ng/mL and from 1.6 to 6.5 ng/mL, respectively. Plasma concentrations for clindamycin generally did not exceed 3.5 ng/mL, with the exception of one subject whose plasma concentration reached 13.1 ng/mL.
Microbiology
Clindamycin binds to the 50S ribosomal subunits of susceptible bacteria and prevents elongation of peptide chains by interfering with peptidyl transfer, thereby suppressing bacterial protein synthesis. Clindamycin has been shown to have in vitro activity against Propionibacterium acnes , an organism which has been associated with acne vulgaris; however, the clinical significance of this activity against P. acnes was not examined in clinical trials with Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel. P. acnes resistance to clindamycin has been documented. Resistance to clindamycin is often associated with resistance to erythromycin.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity, mutagenicity and impairment of fertility testing of Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel have not been performed in any species.
Clindamycin
The carcinogenicity of a 1% clindamycin phosphate gel similar to Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel was evaluated by daily application to mice for 2 years. The daily doses used in this study were approximately 13 and 72 times higher than the human dose of clindamycin phosphate from Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel, assuming complete absorption and based on body surface area comparison. No significant increase in tumors was noted in the treated animals. For purposes of comparisons of the animal exposure to human exposure, the recommended human topical clinical dose is defined as 1 g of Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel applied daily to a 60 kg person.
Fertility (Segment 1) studies in rats treated orally with up to 300 mg/kg/day of clindamycin (approximately 290 times the amount of clindamycin delivered from the recommended clinical dose for Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel, based on body surface area comparison) revealed no effects on fertility or mating ability.
Tretinoin
In two independent studies with long-term topical application of tretinoin in mice, carcinogenicity was not observed. In both studies, tretinoin was administered topically (0.025% or 0.1%) three times per week for up to 2 years. No carcinogenicity was observed with maximum effects of dermal amyloidosis in the basal layer of the skin.
Tretinoin has been shown to enhance photo co-carcinogenicity in properly performed specific studies, employing concurrent or intercurrent exposure to the drug and UV radiation. The contribution of clindamycin to that effect is unknown. Although the significance of these studies to humans is not clear, patients should minimize exposure to sun.
The genotoxic potential of tretinoin was evaluated in an in vitro Ames Salmonella reversion test and an in vitro chromosomal aberration assay in Chinese hamster ovary cells. Both tests were negative.
In oral Segment 1 studies in rats treated with tretinoin, the no-observed-effect-level was 2 mg/kg/day (~78 times the recommended clinical dose assuming 100% absorption and based on body surface area comparison).
CLINICAL STUDIES
The safety and efficacy of once daily use of Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel for treatment of acne vulgaris were assessed in three 12-week prospective, multi-center, randomized, blinded studies in patients 12 years and older. Studies 1 and 2 were of identical design, and compared Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel to clindamycin in the vehicle gel, tretinoin in the vehicle gel, and the vehicle gel alone. Patients with mild, moderate, or severe acne were enrolled in the studies. The co-primary efficacy variables were:
- Mean percent change from baseline at Week 12 in
- inflammatory lesion counts,
- non-inflammatory lesion counts, and
- total lesion counts
- Percent of subjects who cleared or almost cleared at Week 12 as judged by an Evaluator’s Global Severity (EGS) score.
The EGS scoring scale used in all of the clinical trials for Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel is as follows:
| Grade | Description |
|---|---|
Clear | Normal, clear skin with no evidence of acne vulgaris |
Almost Clear | Rare non-inflammatory lesions present, with rare non-inflamed papules (papules must be resolving and may be hyperpigmented, though not pink-red) |
Mild | Some non-inflammatory lesions are present, with few inflammatory lesions (papules/pustules only; no nodulocystic lesions) |
Moderate | Non-inflammatory lesions predominate, with multiple inflammatory lesions evident: several to many comedones and papules/pustules, and there may or may not be one small nodulo-cystic lesion |
Severe | Inflammatory lesions are more apparent, many comedones and papules/pustules, there may or may not be a few nodulocystic lesions |
Very Severe | Highly inflammatory lesions predominate, variable number of comedones, many papules/pustules and many nodulocystic lesions |
In Study 1, a total of 1252 patients were enrolled, and in Study 2, a total of 1288 patients were enrolled. The combined results are presented in Table 3.
| Clindamycin Phosphate 1.2% and Tretinoin 0.025%Gel N=845 | Clindamycin N=426 | Tretinoin N=846 | Vehicle N=423 | |
|---|---|---|---|---|
Evaluator’s Global Severity: N (%) | ||||
Patients achieving success Success was defined as cleared or almost cleared at Week 12. | 180 (21%) | 70 (16%) | 122 (14%) | 34 (8%) |
Inflammatory Lesion Count (% reduction from baseline) | ||||
Mean | 48% | 42% | 39% | 26% |
Non-inflammatory Lesion Count (% reduction from baseline) | ||||
Mean | 36% | 27% | 31% | 16% |
Total Lesion Count (% reduction from baseline) | ||||
Mean | 41% | 34% | 34% | 20% |
In Study 3, Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel was compared to clindamycin gel in a total of 2010 patients with moderate or severe acne vulgaris (see TABLE 3 ). As with Studies 1 and 2, the co-primary endpoints were mean percent reduction in lesion counts (inflammatory, non-inflammatory and total) and the EGS score. In Study 3, success on the EGS score was assessed by the percentage of subjects who had at least 2 grades of improvement from Baseline to Week 12.
| Clindamycin Phosphate 1.2% and Tretinoin 0.025%Gel N=1008 | Clindamycin N=1002 | |
|---|---|---|
Evaluator’s Global Severity: N (%) | ||
Patients achieving success Success was defined as at least a 2-grade improvement at Week 12 from baseline. | 415 (41%) | 345 (34%) |
Inflammatory Lesion Count (% reduction from baseline) | ||
Mean | 61% | 55% |
Non-inflammatory Lesion Count (% reduction from baseline) | ||
Mean | 50% | 41% |
Total Lesion Count (% reduction from baseline) | ||
Mean | 54% | 47% |
HOW SUPPLIED/STORAGE AND HANDLING
Clindamycin Phosphate 1.2% and Tretinoin 0.025% Gel is supplied as follows: 30 gram tube NDC 68682-300-30 60 gram tube NDC 68682-300-60
Storage and Handling
- Store at 25°C (77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature].
- Protect from light.
- Protect from freezing.
- Keep out of the reach of children.
- Keep away from heat.
- Keep tube tightly closed.
Mechanism of Action
Clindamycin
[See Microbiology (12.4) .]
Tretinoin
Although the exact mode of action of tretinoin is unknown, current evidence suggests that topical tretinoin decreases cohesiveness of follicular epithelial cells with decreased microcomedo formation.
Additionally, tretinoin stimulates mitotic activity and increased turnover of follicular epithelial cells causing extrusion of the comedones.