Get your patient on Clindamycin Phosphate And Benzoyl Peroxide - Clindamycin Phosphate And Benzoyl Peroxide gel (Clindamycin Phosphate And Benzoyl Peroxide)
Clindamycin Phosphate And Benzoyl Peroxide - Clindamycin Phosphate And Benzoyl Peroxide gel prescribing information
INDICATIONS AND USAGE
Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% is indicated for the topical treatment of acne vulgaris in patients 12 years or older.
DOSAGE AND ADMINISTRATION
Apply a pea-sized amount of Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% to the face once daily. Use of Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% beyond 12 weeks has not been evaluated.
Concomitant topical acne therapy should be used with caution because a possible cumulative irritancy effect may occur, especially with the use of peeling, desquamating, or abrasive agents. Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% is not for oral, ophthalmic, or intravaginal use.
DOSAGE FORMS AND STRENGTHS
Gel, 1.2% / 2.5% Each gram of Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% contains 10 mg (1%) clindamycin as phosphate, and 25 mg (2.5%) benzoyl peroxide in a white to off-white, opaque, smooth gel.
USE IN SPECIFIC POPULATIONS
Pregnancy
Pregnancy Category C. There are no adequate and well-controlled studies in pregnant women treated with Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5%. Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Animal reproductive/developmental toxicity studies have not been conducted with Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% or benzoyl peroxide. Developmental toxicity studies of clindamycin performed in rats and mice using oral doses of up to 600 mg/kg/day (240 and 120 times amount of clindamycin in the highest recommended adult human dose based on mg/m 2 , respectively) or subcutaneous doses of up to 200 mg/kg/day (80 and 40 times the amount of clindamycin in the highest recommended adult human dose based on mg/m 2 , respectively) revealed no evidence of teratogenicity.
Nursing Mothers
It is not known whether clindamycin is excreted in human milk after topical application of Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5%. However, orally and parenterally administered clindamycin has been reported to appear in breast milk. Because of the potential for serious adverse reactions in nursing infants, a decision should be made whether to use Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% while nursing, taking into account the importance of the drug to the mother.
Pediatric Use
Safety and effectiveness of Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% in pediatric patients under the age of 12 have not been evaluated.
Geriatric Use
Clinical trials of Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% did not include sufficient numbers of subjects aged 65 and older to determine whether they respond differently from younger subjects.
CONTRAINDICATIONS
Clindamycin Phosphate and Benzoyl Peroxide Gel,1.2% / 2.5% is contraindicated in: • Patients who have demonstrated hypersensitivity (e.g., anaphylaxis) to clindamycin, benzoyl peroxide, any components of the formulation, or lincomycin. (4) • Patients with a history of regional enteritis, ulcerative colitis, or antibiotic–associated colitis. (4)
Hypersensitivity
Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% is contraindicated in those individuals who have shown hypersensitivity to clindamycin, benzoyl peroxide, any components of the formulation, or lincomycin. Anaphylaxis, as well as allergic reactions leading to hospitalization, has been reported in postmarketing use with Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5%. [ See Postmarketing Experience (6.2 ) .]
Colitis/Enteritis
Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% is contraindicated in patients with a history of regional enteritis, ulcerative colitis, or antibiotic-associated colitis. [ see Warnings and Precautions (5.1 ) ].
WARNINGS AND PRECAUTIONS
• Colitis: Orally and parenterally administered clindamycin has been associated with severe colitis, which may result in death. Diarrhea, bloody diarrhea, and colitis (including pseudomembranous colitis) have been reported with the use of topical and systemic clindamycin. Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% should be discontinued if significant diarrhea occurs. (5.1) • Ultraviolet Light and Environmental Exposure: Minimize sun exposure following drug application. (5.2)
Colitis
Systemic absorption of clindamycin has been demonstrated following topical use of clindamycin. Diarrhea, bloody diarrhea, and colitis (including pseudomembranous colitis) have been reported with the use of topical and systemic clindamycin. When significant diarrhea occurs, Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% should be discontinued.
Severe colitis has occurred following oral and parenteral administration of clindamycin with an onset of up to several weeks following cessation of therapy. Antiperistaltic agents such as opiates and diphenoxylate with atropine may prolong and/or worsen severe colitis. Severe colitis may result in death.
Studies indicate toxin(s) produced by Clostridia is one primary cause of antibiotic-associated colitis. The colitis is usually characterized by severe persistent diarrhea and severe abdominal cramps and may be associated with the passage of blood and mucus. Stool cultures for Clostridium difficile and stool assay for C. difficile toxin may be helpful diagnostically.
Ultraviolet Light and Environmental Exposure
Minimize sun exposure including use of tanning beds or sun lamps following drug application [ See Nonclinical Toxicology (13.1 ) ].
ADVERSE REACTIONS
The following selected adverse reactions occurred in less than 0.2% of patients: application site pain (0.1%); application site exfoliation (0.1%); and application site irritation (0.1%). (6.1) To report SUSPECTED ADVERSE REACTIONS, contact Encube Ethicals Private Limited at 1-833-285-4151 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch
Clinical Trials Experience
Because clinical trials are conducted under prescribed conditions, adverse reaction rates observed in the clinical trial may not reflect the rates observed in practice. Because clinical trials are also conducted under widely varying conditions, adverse reactions observed in the clinical trials of a drug cannot always be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The following selected adverse reactions occurred in less than 0.2% of patients treated with Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5%: application site pain (0.1%); application site exfoliation (0.1%); and application site irritation (0.1%).
During clinical trials, subjects were assessed for local cutaneous signs and symptoms of erythema, scaling, itching, burning and stinging. Most local skin reactions increased and peaked around week 4 and continually decreased over time reaching near baseline levels by week 12. The percentage of subjects that had symptoms present before treatment, the maximum value recorded during treatment, and the percent with symptoms present at week 12 are shown in Table 1.
Table 1: Local Skin Reactions - Percent of Subjects with Symptoms Present. Combined Results from the Two Phase 3 Trials (N = 773)
| Before Treatment (Baseline) | Maximum During Treatment | End of Treatment (Week 12) | |||||||
| Mild Mod.• Severe | Mild Mod.• Severe | Mild Mod.• Severe | |||||||
| Erythema | 22 | 4 | 0 | 25 | 5 | <1 | 15 | 2 | 0 |
| Scaling | 8 | <1 | 0 | 18 | 3 | 0 | 8 | 1 | 0 |
| Itching | 10 | 2 | 0 | 15 | 2 | 0 | 6 | <1 | 0 |
| Burning | 3 | <1 | 0 | 8 | 2 | 0 | 2 | <1 | 0 |
| Stinging | 2 | <1 | 0 | 6 | 1 | 0 | 1 | <1 | 0 |
•Mod. = Moderate
Postmarketing Experience
Anaphylaxis, as well as allergic reactions leading to hospitalizations, has been reported in postmarketing use of products containing clindamycin/benzoyl peroxide. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
DRUG INTERACTIONS
• Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% should not be used in combination with erythromycin containing products because of its clindamycin component. (7.1)
Erythromycin
Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% should not be used in combination with topical or oral erythromycin-containing products due to its clindamycin component. In vitro studies have shown antagonism between erythromycin and clindamycin. The clinical significance of this in vitro antagonism is not known.
Neuromuscular Blocking Agents
Clindamycin has been shown to have neuromuscular blocking properties that may enhance the action of other neuromuscular blocking agents. Therefore, Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% should be used with caution in patients receiving such agents.
DESCRIPTION
Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% is a combination product with two active ingredients in a white to off-white, opaque, smooth, aqueous gel formulation intended for topical use. Clindamycin phosphate is a water-soluble ester of the semi-synthetic antibiotic produced by a 7(S)-chloro-substitution of the 7(R)-hydroxyl group of the parent antibiotic lincomycin.
The chemical name for clindamycin phosphate is Methyl 7 chloro-6,7,8-trideoxy- 6-(1-methyl-trans-4-propyl-L-2-pyrrolidinecarboxamido)-1-thio-L-threo a-D-galacto octopyranoside 2- (dihydrogen phosphate). The structural formula for clindamycin phosphate is represented below: Clindamycin phosphate:
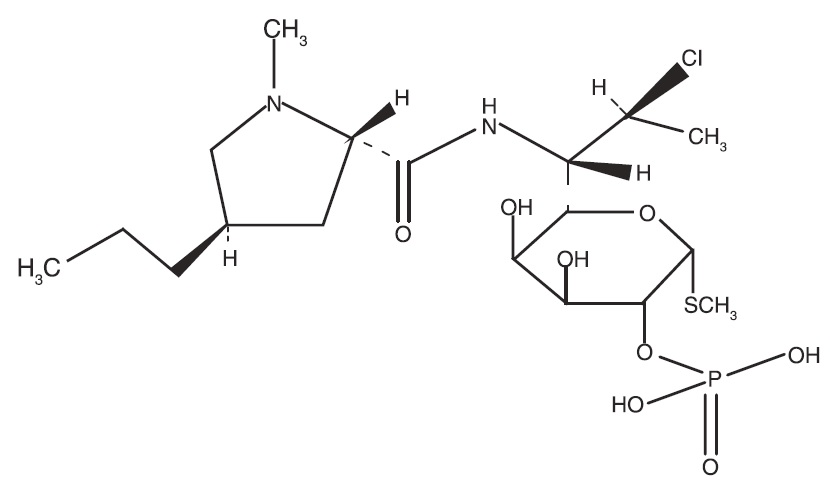
Molecular Formula: C 18 H 34 CIN 2 O 8 PS Molecular Weight: 504.97
Benzoyl peroxide is an antibacterial and keratolytic agent. The structural formula for benzoyl peroxide is represented below: Benzoyl peroxide:
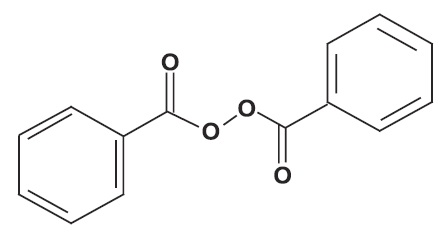
Molecular Formula: C 14 H 10 O 4 Molecular Weight: 242.23
Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% contains the following inactive ingredients: carbopol 980, poloxamer 182, polysorbate 80, propylene glycol, purified water and sodium hydroxide. Each gram of Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% contains 1.2% of clindamycin phosphate which is equivalent to 1% clindamycin.
CLINICAL PHARMACOLOGY
Mechanisms of Action
Clindamycin : Clindamycin is a lincosamide antibacterial [ See Microbiology (12.4 ) ]. Benzoyl Peroxide: Benzoyl peroxide is an oxidizing agent with bacteriocidal and keratolytic effects but the precise mechanism of action is unknown.
Pharmacokinetics
The systemic absorption of clindamycin was investigated in an open-label, multiple-dose trial in 16 adult subjects with moderate to severe acne vulgaris treated with 1 gram of Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% applied to the face once daily for 30 days. Twelve subjects (75%) had at least one quantifiable clindamycin plasma concentration above the lower limit of quantification (LOQ = 0.5 ng/mL) on Day 1 or Day 30. On Day 1, the mean (± standard deviation) peak plasma concentration (C max ) was 0.78 ± 0.22 ng/mL max (n=9 with measurable concentrations), and the mean AUC 0-t was 5.29 ± 0.81 0-t h.ng/mL (n=4). On Day 30, the mean C max was 1.22 ± 0.88 ng/mL (n=10), and the max mean AUC 0-t was 8.42 ± 6.01 h.ng/mL (n=6). Clindamycin plasma concentrations were below LOQ in all subjects at 24 hours post-dose on the three tested days (Day 1, 15, and 30). Benzoyl peroxide has been shown to be absorbed by the skin where it is converted to benzoic acid.
Microbiology
Clindamycin binds to the 50S ribosomal subunits of susceptible bacteria and prevents elongation of peptide chains by interfering with peptidyl transfer, thereby suppressing bacterial protein synthesis.
Clindamycin and benzoyl peroxide individually have been shown to have in vitro activity against Propionibacterium acnes , an organism which has been associated with acne vulgaris; however, the clinical significance of this activity against P. acnes is not known.
P. acnes resistance to clindamycin has been documented. Resistance to clindamycin is often associated with resistance to erythromycin.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity, mutagenicity and impairment of fertility testing of Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% have not been performed. Benzoyl peroxide has been shown to be a tumor promoter and progression agent in a number of animal studies. Benzoyl peroxide in acetone at doses of 5 and 10 mg administered topically twice per week for 20 weeks induced skin tumors in transgenic Tg.AC mice. The clinical significance of this is unknown. Carcinogenicity studies have been conducted with a gel formulation containing 1% clindamycin and 5% benzoyl peroxide. In a 2-year dermal carcinogenicity study in mice, treatment with the gel formulation at doses of 900, 2700, and 15000 mg/kg/day (1.8, 5.4, and 30 times amount of clindamycin and 3.6, 10.8, and 60 times amount of benzoyl peroxide in the highest recommended adult human dose of 2.5 g Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% based on mg/m2, respectively) did not cause any increase in tumors. However, topical treatment with a different gel formulation containing 1% clindamycin and 5% benzoyl peroxide at doses of 100, 500, and 2000 mg/kg/day caused a dose-dependent increase in the incidence of keratoacanthoma at the treated skin site of male rats in a 2-year dermal carcinogenicity study in rats. In an oral (gavage) carcinogenicity study in rats, treatment with the gel formulation at doses of 300, 900 and 3000 mg/kg/day (1.2, 3.6, and 12 times amount of clindamycin and 2.4, 7.2, and 24 times amount of benzoyl peroxide in the highest recommended adult human dose of 2.5 g Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% based on mg/m2, respectively) for up to 97 weeks did not cause any increase in tumors. In a 52-week dermal photocarcinogenicity study in hairless mice, (40 weeks of treatment followed by 12 weeks of observation), the median time to onset of skin tumor formation decreased and the number of tumors per mouse increased relative to controls following chronic concurrent topical administration of the higher concentration benzoyl peroxide formulation (5000 and 10000 mg/kg/day, 5 days/week) and exposure to ultraviolet radiation. Clindamycin phosphate was not genotoxic in the human lymphocyte chromosome aberration assay. Benzoyl peroxide has been found to cause DNA strand breaks in a variety of mammalian cell types, to be mutagenic in S. typhimurium tests by some but not all investigators, and to cause sister chromatid exchanges in Chinese hamster ovary cells. Fertility studies have not been performed with Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% or benzoyl peroxide, but fertility and mating ability have been studied with clindamycin. Fertility studies in rats treated orally with up to 300 mg/kg/day of clindamycin (approximately 120 times the amount of clindamycin in the highest recommended adult human dose of 2.5 g Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5%, based on mg/m 2 ) revealed no effects on fertility or mating ability.
CLINICAL STUDIES
The safety and efficacy of once daily use of Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% were assessed in two 12-week multi center, randomized, blinded trials in subjects 12 years and older with moderate to severe acne vulgaris. The two trials were identical in design and compared Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% to clindamycin in the vehicle gel, benzoyl peroxide in the vehicle gel, and the vehicle gel alone.
The co-primary efficacy variables were:
(1) Mean absolute change from baseline at week 12 in • Inflammatory lesion counts • Non-inflammatory lesion counts
(2) Percent of subjects who had a two grade improvement from baseline on an Evaluator's Global Severity (EGS) score.
The EGS scoring scale used in all of the clinical trials for Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% is as follows:
| Grade | Description |
| Clear | Normal, clear skin with no evidence of acne vulgaris |
| Almost Clear | Rare non-inflammatory lesions present, with rare non-inflamed papules (papules must be resolving and may be hyperpigmented, though not pink-red) |
| Mild | Some non-inflammatory lesions are present, with few inflammatory lesions (papules/pustules only; no nodulocystic lesions) |
| Moderate | Non-inflammatory lesions predominate, with multiple inflammatory lesions evident: several to many comedones and papules/pustules, and there may or may not be one small nodulo-cystic lesion |
| Severe | Inflammatory lesions are more apparent, many comedones and papules/pustules, there may or may not be a few nodulocystic lesions |
| Very Severe | Highly inflammatory lesions predominate, variable number of comedones, many papules/pustules and many nodulocystic lesions |
The results of Trial 1 at week 12 are presented in Table 2: Table 2: Trial 1 Results
| Trial 1 | Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% N = 399 | Clindamycin Gel N = 408 | Benzoyl Peroxide Gel N = 406 | Vehicle Gel N = 201 |
| EGSS Clear or Almost Clear 2 grade reduction from baseline | 115 (29%) 131 (33%) | 84 (21%) 100 (25%) | 76 (19%) 96 (24%) | 29 (14%) 38 (19%) |
| Inflammatory Lesions: Mean absolute change Mean percent (%) reduction | 14.8 55.0% | 12.2 47.1% | 13.0 49.3% | 9.0 34.5% |
| Non-Inflammatory Lesions: Mean absolute change Mean percent (%) reduction | 22.1 45.3% | 17.9 38.0% | 20.6 40.2% | 13.2 28.6% |
The results of Trial 2 at week 12 are presented in Table 3:
Table 3: Trial 2 Results
| Trial 2 | Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% N = 398 | Clindamycin Gel N = 404 | Benzoyl Peroxide Gel N = 403 | Vehicle Gel N = 194 |
| EGSS Clear or Almost Clear 2 grade reduction from baseline | 113 (28%) 147 (37%) | 94 (23%) 114 (28%) | 94 (23%) 114 (28%) | 21 (11%) 27 (14%) |
| Inflammatory Lesions: Mean absolute change Mean percent (%) reduction | 13.7 54.2% | 11.3 45.3% | 11.2 45.7% | 5.7 23.3% |
| Non-Inflammatory Lesions: Mean absolute change Mean percent (%) reduction | 19.0 41.2% | 14.9 34.3% | 15.2 34.5% | 8.3 19.2% |
HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% is supplied as a 50 g pump (NDC 21922-074-40).
Dispensing Instructions for the Pharmacist
• Dispense Clindamycin Phosphate and Benzoyl Peroxide Gel, 1.2% / 2.5% with a 10 week expiration date. • Specify “Store at room temperature up to 25°C (77°F). Do not freeze.”
Storage and Handling
• PHARMACIST: Prior to Dispensing: Store in a refrigerator, 2°C to 8°C (36°F to 46°F). • PATIENT: Store at room temperature at or below 25°C (77°F). • Protect from freezing. • Keep out of the reach of children. • Keep container tightly closed.
Mechanisms of Action
Clindamycin : Clindamycin is a lincosamide antibacterial [ See Microbiology (12.4 ) ]. Benzoyl Peroxide: Benzoyl peroxide is an oxidizing agent with bacteriocidal and keratolytic effects but the precise mechanism of action is unknown.