Clorazepate Dipotassium - Clorazepate Dipotassium tablet prescribing information
WARNING: RISKS FROM CONCOMITANT USE WITH OPIOIDS; ABUSE, MISUSE, AND ADDICTION; and DEPENDENCE AND WITHDRAWAL REACTIONS
- Concomitant use of benzodiazepines and opioids may result in profound sedation, respiratory depression, coma, and death. Reserve concomitant prescribing of these drugs in patients for whom alternative treatment options are inadequate. Limit dosages and durations to the minimum required. Follow patients for signs and symptoms of respiratory depression and sedation (See WARNINGS and PRECAUTIONS ).
- The use of benzodiazepines, including clorazepate dipotassium, exposes users to risks of abuse, misuse, and addiction, which can lead to overdose or death. Abuse and misuse of benzodiazepines commonly involve concomitant use of other medications, alcohol, and/or illicit substances, which is associated with an increased frequency of serious adverse outcomes. Before prescribing clorazepate dipotassium and throughout out treatment, assess each patient’s risk for abuse, misuse, and addiction (See WARNINGS ).
- The continued use of benzodiazepines, including clorazepate dipotassium, may lead to clinically significant physical dependence. The risks of dependence and withdrawal increase with longer treatment duration and higher daily dose. Abrupt discontinuation or rapid dosage reduction of clorazepate dipotassium after continued use may precipitate acute withdrawal reactions, which can be life-threatening. To reduce the risk of withdrawal reactions, use a gradual taper to discontinue clorazepate dipotassium or reduce the dosage (See DOSAGE AND ADMINISTRATION and WARNINGS ).
INDICATIONS AND USAGE
Clorazepate dipotassium tablets are indicated for the management of anxiety disorders or for the short-term relief of the symptoms of anxiety. Anxiety or tension associated with the stress of everyday life usually does not require treatment with an anxiolytic.
Clorazepate dipotassium tablets are indicated as adjunctive therapy in the management of partial seizures.
The effectiveness of clorazepate dipotassium tablets in long-term management of anxiety, that is, more than 4 months, has not been assessed by systematic clinical studies. Long-term studies in epileptic patients, however, have shown continued therapeutic activity. The physician should reassess periodically the usefulness of the drug for the individual patient.
Clorazepate dipotassium tablets are indicated for the symptomatic relief of acute alcohol withdrawal.
DOSAGE AND ADMINISTRATION
For the Symptomatic Relief of Anxiety: Clorazepate dipotassium tablets are administered orally in divided doses. The usual daily dose is 30 mg. The dose should be adjusted gradually within the range of 15 to 60 mg daily in accordance with the response of the patient. In elderly or debilitated patients it is advisable to initiate treatment at a daily dose of 7.5 to 15 mg.
Clorazepate dipotassium tablets may also be administered in a single dose daily at bedtime; the recommended initial dose is 15 mg. After the initial dose, the response of the patient may require adjustment of subsequent dosage. Lower doses may be indicated in the elderly patient. Drowsiness may occur at the initiation of treatment and with dosage increment.
For the Symptomatic Relief of Acute Alcohol Withdrawal:
The following dosage schedule is recommended:
| 1st 24 hours (Day 1) | 30 mg initially; followed by 30 to 60 mg in divided doses |
| 2nd 24 hours (Day 2) | 45 to 90 mg in divided doses |
| 3rd 24 hours (Day 3) | 22.5 to 45 mg in divided doses |
| Day 4 | 15 to 30 mg in divided doses |
Thereafter, gradually reduce the daily dose to 7.5 to 15 mg. Discontinue drug therapy as soon as patient’s condition is stable.
The maximum recommended total daily dose is 90 mg. Avoid excessive reductions in the total amount of drug administered on successive days.
As an Adjunct to Antiepileptic Drugs: In order to minimize drowsiness, the recommended initial dosages and dosage increments should not be exceeded.
Adults: The maximum recommended initial dose in patients over 12 years old is 7.5 mg three times a day. Dosage should be increased by no more than 7.5 mg every week and should not exceed 90 mg/day.
Children (9 to 12 years): The maximum recommended initial dose is 7.5 mg two times a day. Dosage should be increased by no more than 7.5 mg every week and should not exceed 60 mg/day.
Discontinuation or Dosage Reduction of Clorazepate Dipotassium Tablets: To reduce the risk of withdrawal reactions, use a gradual taper to discontinue clorazepate dipotassium tablets or reduce the dosage. If a patient develops withdrawal reactions, consider pausing the taper or increasing the dosage to the previous tapered dosage level. Subsequently decrease the dosage more slowly (see WARNINGS and DRUG ABUSE AND DEPENDENCE ).
CONTRAINDICATIONS
Clorazepate dipotassium tablets are contraindicated in patients with a known hypersensitivity to the drug and in those with acute narrow angle glaucoma.
ADVERSE REACTIONS
The side effect most frequently reported was drowsiness. Less commonly reported (in descending order of occurrence) were: dizziness, various gastrointestinal complaints, nervousness, blurred vision, dry mouth, headache, and mental confusion. Other side effects included insomnia, transient skin rashes, fatigue, ataxia, genitourinary complaints, irritability, diplopia, depression, tremor, and slurred speech.
There have been reports of abnormal liver and kidney function tests and of decrease in hematocrit.
Decrease in systolic blood pressure has been observed.
To report SUSPECTED ADVERSE REACTIONS, contact Aurobindo Pharma USA, Inc. at 1-866-850-2876 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch .
DRUG INTERACTIONS
The concomitant use of benzodiazepines and opioids increases the risk of respiratory depression because of actions at different receptor sites in the CNS that control respiration. Benzodiazepines interact at GABAA sites and opioids interact primarily at mu receptors. When benzodiazepines and opioids are combined, the potential for benzodiazepines to significantly worsen opioid-related respiratory depression exists. Limit dosage and duration of concomitant use of benzodiazepines and opioids, and monitor patients closely for respiratory depression and sedation.
If clorazepate dipotassium is to be combined with other drugs acting on the central nervous system, careful consideration should be given to the pharmacology of the agents to be employed. Animal experience indicates that clorazepate dipotassium prolongs the sleeping time after hexobarbital or after ethyl alcohol, increases the inhibitory effects of chlorpromazine, but does not exhibit monoamine oxidase inhibition. Clinical studies have shown increased sedation with concurrent hypnotic medications. The actions of the benzodiazepines may be potentiated by barbiturates, narcotics, phenothiazines, monoamine oxidase inhibitors or other antidepressants.
If clorazepate dipotassium tablets are used to treat anxiety associated with somatic disease states, careful attention must be paid to possible drug interaction with concomitant medication.
In bioavailability studies with normal subjects, the concurrent administration of antacids at therapeutic levels did not significantly influence the bioavailability of clorazepate dipotassium tablets.
DESCRIPTION
Chemically, clorazepate dipotassium is a benzodiazepine. The empirical formula is C 16 H 11 ClK 2 N 2 O 4 ; the molecular weight is 408.92; 1 H -1, 4 Benzodiazepine-3-carboxylic acid, 7-chloro-2,3-dihydro-2-oxo-5-phenyl-, potassium salt compound with potassium hydroxide (1:1) and the structural formula may be represented as follows:
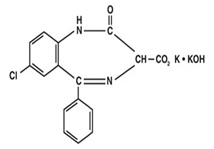
The compound occurs as a fine, white or light yellow crystalline powder. It is insoluble in the common organic solvents, but very soluble in water. Aqueous solutions are unstable, clear, light yellow, and alkaline.
Clorazepate dipotassium tablets, USP contain 3.75 mg, 7.5 mg or 15 mg of clorazepate dipotassium, USP for oral administration. Inactive ingredients for clorazepate dipotassium tablets: croscarmellose sodium, magnesium oxide, magnesium stearate, microcrystalline cellulose, potassium carbonate, sodium chloride and sodium lauryl sulfate. The 3.75 mg tablets also contain FD&C Blue No. 2 Aluminum Lake and the 7.5 mg tablets also contain FD&C Yellow No. 6 Aluminum Lake.
CLINICAL PHARMACOLOGY
Pharmacologically, clorazepate dipotassium has the characteristics of the benzodiazepines. It has depressant effects on the central nervous system. The primary metabolite, nordiazepam, quickly appears in the blood stream. The serum half-life is about 2 days. The drug is metabolized in the liver and excreted primarily in the urine.
Studies in healthy men have shown that clorazepate dipotassium has depressant effects on the central nervous system. Prolonged administration of single daily doses as high as 120 mg was without toxic effects. Abrupt cessation of high doses was followed in some patients by nervousness, insomnia, irritability, diarrhea, muscle aches, or memory impairment.
Since orally administered clorazepate dipotassium is rapidly decarboxylated to form nordiazepam, there is essentially no circulating parent drug. Nordiazepam, the primary metabolite, quickly appears in the blood and is eliminated from the plasma with an apparent half-life of about 40 to 50 hours. Plasma levels of nordiazepam increase proportionally with clorazepate dipotassium dose and show moderate accumulation with repeated administration. The protein binding of nordiazepam in plasma is high (97 to 98%).
Within 10 days after oral administration of a 15 mg (50 µCi) dose of 14 C-clorazepate dipotassium to two volunteers, 62 to 67% of the radioactivity was excreted in the urine and 15 to 19% was eliminated in the feces. Both subjects were still excreting measurable amounts of radioactivity in the urine (about 1% of the 14 C-dose) on day ten.
Nordiazepam is further metabolized by hydroxylation. The major urinary metabolite is conjugated oxazepam (3-hydroxynordiazepam), and smaller amounts of conjugated p-hydroxynordiazepam and nordiazepam are also found in the urine.
HOW SUPPLIED
Clorazepate Dipotassium Tablets, USP are available containing 3.75 mg, 7.5 mg or 15 mg of clorazepate dipotassium, USP.
The 3.75 mg tablets are mottled blue colored, round, flat face tablets, debossed with "CL" and "11" separated by score-line on one side and plain on other side. They are available as follows:
Bottles of 100 NDC 13107-282-01 Bottles of 500 NDC 13107-282-05
The 7.5 mg tablets are mottled peach colored, round, flat face tablets, debossed with "CL" and "14" separated by score-line on one side and plain on other side.They are available as follows:
Bottles of 100 NDC 13107-283-01 Bottles of 500 NDC 13107-283-05
The 15 mg tablets are mottled white to off white colored, round, flat face tablets, debossed with "CL" and "17" separated by score-line on one side and plain on other side. They are available as follows:
Bottles of 100 NDC 13107-284-01
Store at 20° to 25°C (68° to 77°F). [See USP Controlled Room Temperature.]
Protect from light and moisture.
Dispense in a tight, light-resistant container as defined in the USP using a child-resistant closure.
PHARMACIST: Dispense a Medication Guide with each prescription.
Dispense with Medication Guide available at: www.aurobindousa.com/medication-guides
Distributed by: Aurobindo Pharma USA, Inc. 279 Princeton-Hightstown Road East Windsor, NJ 08520 Manufactured by: Aurobindo Pharma Limited Hyderabad-500 032, India Revised: 09/2023 Dispense with Medication Guide available at: www.aurobindousa.com/medication-guides