Get your patient on Cyanocobalamin - Cyanocobalamin spray, Metered (Cyanocobalamin)
Cyanocobalamin - Cyanocobalamin spray, Metered prescribing information
INDICATIONS AND USAGE
Cyanocobalamin Nasal Spray is indicated for:
- Vitamin B12 maintenance therapy in adult patients with pernicious anemia who are in remission following intramuscular vitamin B12 therapy and who have no nervous system involvement
- Treatment of adult patients with dietary, drug-induced, or malabsorption-related vitamin B12 deficiency not due to pernicious anemia
- Prevention of vitamin B12 deficiency in adult patients with vitamin B12 requirements in excess of normal
Limitations of Use:
- Cyanocobalamin Nasal Spray should not be used for the vitamin B12 absorption test (Schilling test).
- In patients with correctible or temporary causes of vitamin B12 deficiency, the benefit of continued long term use of Cyanocobalamin Nasal Spray following adequate correction of vitamin B12 deficiency and underlying disease has not been established.
- The effectiveness of Cyanocobalamin Nasal Spray in patients with active symptoms of nasal congestion, allergic rhinitis or upper respiratory infection has not been determined. Treatment with Cyanocobalamin Nasal Spray should be deferred until symptoms have subsided.
DOSAGE AND ADMINISTRATION
- Prior to treatment, obtain hematocrit, reticulocyte count, vitamin B12, folate, and iron levels. (2.1 )
- The recommended initial dose is one spray (500 mcg) in one nostril once weekly. (2.2 )
- Administer at least one hour before or one hour after ingestion of hot foods or liquids. (2.2 )
- Monitor serum B12 levels periodically. Obtain a serum B12 level and peripheral blood count one month after treatment initiation, then subsequently at intervals of 3 to 6 months. (2.3 )
- If serum levels of B12 decline after one month of treatment, consider increasing the dose. Assess serum B12 level one month after each dose adjustment. If serum B12 levels are persistently low, consider alternative therapy (e.g., intramuscular or subcutaneous vitamin B12 therapy). (2.3 )
- See Full Prescribing Information to see what other therapies should be administered with Cyanocobalamin Nasal Spray. (2.4 )
Testing and Other Considerations Prior to Dosing
Prior to treatment, obtain hematocrit, reticulocyte count, vitamin B12, folate, and iron levels [see Dosage and Administration (2.4) ] . Consider the potential for concomitant drugs to interfere with vitamin B 12 and folate diagnostic blood assays [see Drug Interactions (7) ] .
In patients with suspected cobalamin hypersensitivity, consider administering an intradermal test dose of parenteral vitamin B12 prior to use of Cyanocobalamin Nasal Spray [see Warnings and Precautions (5.2) ] .
Recommended Dosage
The recommended initial dose of Cyanocobalamin Nasal Spray is one spray (500 mcg) administered in ONE nostril once weekly. Administer Cyanocobalamin Nasal Spray at least one hour before or one hour after ingestion of hot foods or liquids since hot foods may cause nasal secretions and a resulting loss of medication. Defer use of Cyanocobalamin Nasal Spray in patients with nasal congestion, allergic rhinitis, or upper respiratory infections until after symptoms have subsided.
Monitoring, Dosage Modifications, and Treatment Duration
Monitoring for Response and Safety
Monitor serum B 12 levels periodically during therapy to establish adequacy of therapy. Obtain a serum B 12 level and peripheral blood count one month after treatment initiation, then subsequently at intervals of 3 to 6 months [see Warnings and Precautions (5.3) ] .
Dosage Modifications
If serum levels of B 12 decline after one month of treatment with Cyanocobalamin Nasal Spray, consider increasing the dose. Assess serum B 12 level one month after each dose adjustment. If serum B 12 levels are persistently low, consider alternative therapy (e.g., intramuscular or subcutaneous vitamin B 12 therapy).
Treatment Duration
In patients whose underlying cause of vitamin B 12 deficiency has been corrected and are deemed no longer at risk for vitamin B 12 deficiency, discontinue Cyanocobalamin Nasal Spray. The safety and effectiveness of continued long-term use in these individuals has not been established.
In patients with pernicious anemia, continue appropriate vitamin B 12 treatment indefinitely.
Administration of Cyanocobalamin Nasal Spray with Other Therapy
- Cyanocobalamin Nasal Spray should be administered with other therapy(ies) in:
- Patients with concurrent folate and vitamin B12 deficiency: Administer folic acid in addition to Cyanocobalamin Nasal Spray
- Patients with concurrent iron and vitamin B12 deficiency: Administer iron in addition to Cyanocobalamin Nasal Spray
- Patients with correctible causes of vitamin B12 deficiency: Consider measures to treat the underlying condition associated with vitamin B12 deficiency in addition to treatment with Cyanocobalamin Nasal Spray
DOSAGE FORMS AND STRENGTHS
Nasal spray: 500 mcg/0.1 mL (per actuation), packaged in a single-use device containing 0.125 mL of solution
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
The limited available data on Cyanocobalamin Nasal Spray in pregnant women are insufficient to inform a drug-associated risk of adverse developmental outcomes. However, vitamin B12 is an essential vitamin and requirements are increased during pregnancy.
Animal reproduction studies have not been conducted with vitamin B12.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. In the U.S. general population, the estimated background risks of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
Lactation
Risk Summary
Vitamin B12 is present in the milk of lactating women in concentrations which approximate the mother's vitamin B12 blood level. Vitamin B12 does not appear to pose more than a minimal risk to breastfeeding children.
Pediatric Use
Safety and effectiveness have not been established in pediatric patients.
Geriatric Use
Clinical studies of Cyanocobalamin Nasal Spray did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients.
CONTRAINDICATIONS
Cyanocobalamin Nasal Spray is contraindicated in patients with hypersensitivity to cobalt and/or vitamin B12 or any of its excipients [see Warnings and Precautions (5.2) ] . Anaphylactic shock and death have been reported after parenteral vitamin B12 administration in sensitive patients.
WARNINGS AND PRECAUTIONS
- Severe Optic Atrophy in Patients with Leber's Disease : Patients with early Leber's disease who were treated with vitamin B12 suffered severe and swift optic atrophy. Cyanocobalamin Nasal Spray is not recommended for use in these patients (5.1 )
- Anaphylactic Reactions : Anaphylactic shock and death have been reported after parenteral vitamin B12 administration. If patients are to start Cyanocobalamin Nasal Spray before having tolerated cyanocobalamin parenterally, consider administering an intradermal test dose of parenteral vitamin B12 to patients suspected of cyanocobalamin hypersensitivity. (2.1 , 5.2 )
- Masking of Folate Deficiency with Vitamin B12 Use : Doses of vitamin B12 exceeding 10 mcg daily may produce hematologic response in patients with folate deficient megaloblastic anemia and may therefore mask a previously unrecognized folate deficiency. Assess both vitamin B12 and folate levels prior to initiating therapy with Cyanocobalamin Nasal Spray or with folic acid. (5.3 )
- Hypokalemia and Thrombocytosis Due to Intense Treatment of Megaloblastic Anemia : Hypokalemia and sudden death may occur in severe megaloblastic anemia that is treated intensely with vitamin B12. Monitor serum potassium levels and platelet count during therapy. (5.4 )
- Unmasking of Polycythemia Vera : Vitamin B12 deficiency may suppress the signs of polycythemia vera. Treatment with Cyanocobalamin Nasal Spray may unmask this condition. Patients exhibiting clinical or hematologic response consistent with polycythemia vera should be referred for further evaluation. (5.5 )
Severe Optic Atrophy in Patients with Leber’s Disease
Patients with early Leber's disease (hereditary optic nerve atrophy) who were treated with vitamin B12 suffered severe and swift optic atrophy. Cyanocobalamin products, including
Cyanocobalamin Nasal Spray, is not recommended for use in patients with Leber's optic atrophy. For patients with Leber's disease requiring vitamin B12, consider alternative therapy (e.g., hydroxocobalamin) for B12 supplementation.
Anaphylactic Reactions
Anaphylactic shock and death have been reported after parenteral vitamin B12 administration. If patients are to start Cyanocobalamin Nasal Spray before having tolerated cyanocobalamin parenterally, consider administering an intradermal test dose of parenteral vitamin B12 to patients suspected of cyanocobalamin hypersensitivity [see Dosage and Administration (2.1) ] .
Masking of Folate Deficiency with Vitamin B12 Use
Doses of vitamin B12 exceeding 10 mcg daily may produce hematologic response in patients with folate deficient megaloblastic anemia and may therefore mask a previously unrecognized folate deficiency. Vitamin B12 is not a substitute for folic acid [see Dosage and Administration (2.4) ] . Assess both vitamin B12 and folate levels prior to initiating therapy with vitamin B12, including Cyanocobalamin Nasal Spray, or with folic acid [see Dosage and Administration (2.1) ] .
Hypokalemia and Thrombocytosis Due to Intense Treatment of Megaloblastic Anemia
Hypokalemia and sudden death may occur in severe megaloblastic anemia that is treated intensely with vitamin B12. Hypokalemia and thrombocytosis can occur upon conversion of severe megaloblastic anemia to normal erythropoiesis with vitamin B12 therapy. Therefore, serum potassium levels and platelet count should be monitored carefully during therapy [see Dosage and Administration (2.3) ] .
Unmasking of Polycythemia Vera
Vitamin B12 deficiency may suppress the signs of polycythemia vera. Treatment with vitamin B12 may unmask this condition. Patients exhibiting clinical or hematologic response consistent with polycythemia vera should be referred for further evaluation.
ADVERSE REACTIONS
The following serious adverse reactions are described elsewhere in the labeling:
- Severe Optic Atrophy in Patients with Leber's Disease [see Warnings and Precautions (5.1) ].
- Anaphylactic Reactions [see Warnings and Precautions (5.2) ].
- Hypokalemia and Thrombocytosis Due to Intense Treatment of Megaloblastic Anemia [see Warnings and Precautions (5.4) ].
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. The adverse reactions
described in Table 1 below are based on data from an eight week cross over trial in which vitamin B12 deficient patients in hematologic remission received one vitamin B12 intramuscular injection (N=25) and then received once weekly intranasal administration of another nasal cyanocobalamin formulation (N=24) for 4 weeks.
| Adverse Reaction | Number of Patients (%) | |
| Another Cyanocobalamin Nasal Formulation, 500 mcg (n=24) | Intramuscular Cyanocobalamin•, 100 mcg (n=25) | |
| Infectiona | 3 (13) | 3 (12) |
| Headache | 1 (4) | 5 (20) |
| Asthenia | 1 (4) | 4 (16) |
| Nausea | 1 (4) | 1 (4) |
| Glossitis | 1 (4) | 0 (0) |
| Paresthesia | 1 (4) | 1 (4) |
| Rhinitis | 1 (4) | 2 (8) |
| a Sore throat, common cold • The data are not an adequate basis for comparison of rates between the study drug and the active control | ||
DRUG INTERACTIONS
Chloramphenicol may decrease the efficacy of Cyanocobalamin Nasal Spray when used for treatment of anemia. If Cyanocobalamin Nasal Spray is used for the treatment of anemia concomitantly with chloramphenicol, monitor for reduced efficacy and if needed, consider an alternative therapy.
DESCRIPTION
Cyanocobalamin is a synthetic form of vitamin B12. The chemical name is 5,6-dimethyl-benzimidazolyl cyanocobamide. The cobalt content is 4.35%. The molecular formula is C 63 H 88 CoN 14 O 14 P, which corresponds to a molecular weight of 1355.38 and the following structural formula:
Figure 1. Cyanocobalamin Chemical Structure
Cyanocobalamin occurs as red to purplish red crystalline powder or small crystals. It is very hygroscopic in the anhydrous form, and sparingly to moderately soluble in water (1:80). Its pharmacologic activity is destroyed by heavy metals (iron) and strong oxidizing or reducing agents (vitamin C), but not by autoclaving for short periods of time (15-20 minutes) at 121°C. The vitamin B 12 coenzymes are very unstable in light.
Cyanocobalamin Nasal Spray is a solution of cyanocobalamin, USP (vitamin B 12 ) for administration as a spray to the nasal mucosa. Each single-use device of Cyanocobalamin Nasal Spray contains 0.125 mL of a 500 mcg/0.1 mL solution of cyanocobalamin with, benzalkonium chloride in purified water, citric acid, glycerin and sodium citrate. The spray solution has a pH between 4.5 and 5.5. Each spray delivers an average of 500 mcg of cyanocobalamin per actuation.
CLINICAL PHARMACOLOGY
Mechanism of Action
Vitamin B 12 can be converted to coenzyme B 12 in tissues, and as such is essential for conversion of methylmalonate to succinate and synthesis of methionine from homocysteine, a reaction which also requires folate. In the absence of coenzyme B 12 , tetrahydrofolate cannot be regenerated from its inactive storage form, 5-methyltetrahydrofolate, and a functional folate deficiency occurs. Vitamin B 12 also may be involved in maintaining sulfhydryl (SH) groups in the reduced form required by many SH-activated enzyme systems. Through these reactions, vitamin B12 is associated with fat and carbohydrate metabolism and protein synthesis.
Pharmacodynamics
Parenteral (intramuscular) administration of vitamin B 12 completely reverses the megaloblastic anemia and GI symptoms of vitamin B 12 deficiency; the degree of improvement in neurologic symptoms depends on the duration and severity of the lesions, although progression of the lesions is immediately arrested. In pernicious anemia patients, once weekly intranasal dosing with 500 mcg B12 gel resulted in a consistent increase in pre-dose serum B12 levels during one month of treatment (p < 0.003) above that seen one month after 100 mcg intramuscular dose (Figure 2).
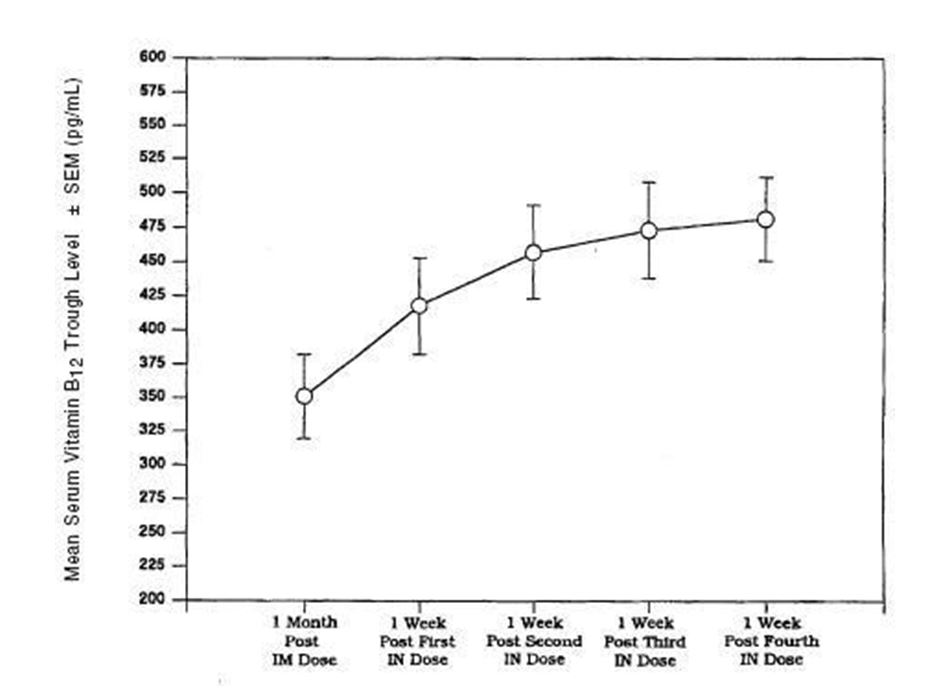
Figure 2. Vitamin B12 Serum Trough Levels After Intramuscular Solution (IM) of 100 mcg and Nasal Gel (IN) Administration of 500 mcg Cyanocobalamin After Weekly Doses.
Pharmacokinetics Absorption
Vitamin B 12 is bound to intrinsic factor during transit through the stomach; separation occurs in the terminal ileum in the presence of calcium, and vitamin B 12 enters the mucosal cell for absorption. It is then transported by the transcobalamin binding proteins. A small amount (approximately 1% of the total amount ingested) is absorbed by simple diffusion, but this mechanism is adequate only with very large doses.
A three way crossover study in 25 fasting healthy subjects was conducted to compare the bioavailability of the B12 nasal spray to the B12 nasal gel and to evaluate the relative bioavailability of the nasal formulations as compared to the intramuscular injection. The peak concentrations after administration of intranasal spray were reached in 1.25 +/
1.9 hours. The mean peak plasma concentration (Cmax) of B12, obtained after baseline correction, following administration of intranasal spray were 748 +/-549 pg/mL.
The bioavailability of the B12 nasal spray was found to be 10% less than the B12 nasal gel.
Distribution
In the blood, B12 is bound to transcobalamin II, a specific B-globulin carrier protein, and is distributed and stored primarily in the liver and bone marrow.
Elimination
About 3-8 mcg of B12 is secreted into the GI tract daily via the bile and undergoes some enterohepatic recycling; in normal subjects with sufficient intrinsic factor, all but about 1 mcg is reabsorbed. When B12 is administered in doses which saturate the binding capacity of plasma proteins and the liver, the unbound B12 is rapidly eliminated in the urine. Retention of B12 in the body is dose-dependent. About 80-90% of an intramuscular dose up to 50 mcg is retained in the body; this percentage drops to 55% for a 100 mcg dose, and decreases to 15% when a 1000 mcg dose is given.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term studies in animals to evaluate carcinogenic potential have not been done.
HOW SUPPLIED/STORAGE AND HANDLING
Cyanocobalamin Nasal Spray is a nasal spray available in a dosage strength of 500 mcg cyanocobalamin/0.1 mL (per actuation). It is supplied in boxes of 4 single-use nasal spray devices and a package insert (NDC 43386-237-70).
Protect from light. Keep covered in carton until ready to use. Store upright at controlled room temperature 15°C to 30°C (59°F to 86°F). Protect from freezing.
Mechanism of Action
Vitamin B 12 can be converted to coenzyme B 12 in tissues, and as such is essential for conversion of methylmalonate to succinate and synthesis of methionine from homocysteine, a reaction which also requires folate. In the absence of coenzyme B 12 , tetrahydrofolate cannot be regenerated from its inactive storage form, 5-methyltetrahydrofolate, and a functional folate deficiency occurs. Vitamin B 12 also may be involved in maintaining sulfhydryl (SH) groups in the reduced form required by many SH-activated enzyme systems. Through these reactions, vitamin B12 is associated with fat and carbohydrate metabolism and protein synthesis.