Get your patient on Disopyramide Phosphate - Disopyramide Phosphate capsule (Disopyramide Phosphate)
Disopyramide Phosphate - Disopyramide Phosphate capsule prescribing information
Mortality
In the National Heart, Lung and Blood Institute's Cardiac Arrhythmia Suppression Trial (CAST), a long-term, multi-center, randomized, double-blind study in patients with asymptomatic non-life threatening ventricular arrhythmias who had had a myocardial infarction more than 6 days but less than 2 years previously, an excessive mortality or nonfatal cardiac arrest rate (7.7%) was seen in patients treated with encainide or flecainide compared with that seen in patients assigned to carefully matched placebo-treated groups (3%). The average duration of treatment with encainide or flecainide in this study was 10 months.
The applicability of the CAST results to other populations (e.g., those without recent myocardial infarction) is uncertain. Considering the known proarrhythmic properties of disopyramide and the lack of evidence of improved survival for any antiarrhythmic drug in patients without life-threatening arrhythmias, the use of disopyramide as well as other antiarrhythmic agents should be reserved for patients with life-threatening ventricular arrhythmias.
INDICATIONS AND USAGE
Disopyramide phosphate capsules are indicated for the treatment of documented ventricular arrhythmias, such as sustained ventricular tachycardia, that, in the judgment of the physician, are life-threatening. Because of the proarrhythmic effects of disopyramide, its use with lesser arrhythmias is generally not recommended. Treatment of patients with asymptomatic ventricular premature contractions should be avoided.
Initiation of disopyramide treatment, as with other antiarrhythmic agents used to treat life-threatening arrhythmias, should be carried out in the hospital.
Antiarrhythmic drugs have not been shown to enhance survival in patients with ventricular arrhythmias.
DOSAGE AND ADMINISTRATION
The dosage of disopyramide (as the phosphate) must be individualized for each patient on the basis of response and tolerance. The usual adult dosage of disopyramide is 400 to 800 mg (calculated as the disopyramide base) per day given in divided doses. The recommended dosage for most adults is 600 mg/day given in divided doses (150 mg every 6 hours). For patients whose body weight is less than 110 pounds (50 kg), the recommended dosage is 400 mg/day given in divided doses (100 mg every 6 hours). In the event of increased anticholinergic side effects, plasma levels of disopyramide should be monitored and the dose of the drug adjusted accordingly. A reduction of the dose by one third, from the recommended 600 mg/day to 400 mg/day, would be reasonable, without changing the dosing interval.
For patients with cardiomyopathy or possible cardiac decompensation, a loading dose, as discussed below, should not be given, and initial dosage should be limited to 100 mg every 6 to 8 hours. Subsequent dosage adjustments should be made gradually, with close monitoring for the possible development of hypotension and/or congestive heart failure (see WARNINGS ).
For patients with moderate renal insufficiency (creatinine clearance greater than 40 mL/min) or hepatic insufficiency, the recommended dosage is 400 mg/day given in divided doses (100 mg every 6 hours).
For patients with severe renal insufficiency (Ccr 40 mL/min or less), the recommended dosage regimen of disopyramide is 100 mg at intervals shown in the table below, with or without an initial loading dose of 150 mg.
| Creatinine clearance (mL/min) | 40-30 | 30-15 | less than 15 |
| Approximate maintenance-dosing interval | q 8 hr | q 12 hr | q 24 hr |
For patients in whom rapid control of ventricular arrhythmia is essential, an initial loading dose of 300 mg disopyramide (200 mg for patients whose body weight is less than 110 pounds) is recommended, followed by the appropriate maintenance dosage. Therapeutic effects are usually attained 30 minutes to 3 hours after administration of a 300 mg loading dose. If there is no response or evidence of toxicity within 6 hours of the loading dose, 200 mg of disopyramide every 6 hours may be prescribed instead of the usual 150 mg. If there is no response to this dosage within 48 hours, either disopyramide should then be discontinued or the physician should consider hospitalizing the patient for careful monitoring while subsequent disopyramide doses of 250 mg or 300 mg every 6 hours are given. A limited number of patients with severe refractory ventricular tachycardia have tolerated daily doses of disopyramide up to 1600 mg per day (400 mg every 6 hours), resulting in disopyramide plasma levels up to 9 mcg/mL. If such treatment is warranted, it is essential that patients be hospitalized for close evaluation and continuous monitoring.
Transferring to Disopyramide Phosphate
The following dosage schedule based on theoretical considerations rather than experimental data is suggested for transferring patients with normal renal function from either quinidine sulfate or procainamide therapy (Type 1 antiarrhythmic agents) to disopyramide therapy:
Disopyramide should be started using the regular maintenance schedule without a loading dose 6 to 12 hours after the last dose of quinidine sulfate or 3 to 6 hours after the last dose of procainamide.
In patients in whom withdrawal of quinidine sulfate or procainamide is likely to produce life-threatening arrhythmias, the physician should consider hospitalization of the patient.
Pediatric Dosage
Controlled clinical studies have not been conducted in pediatric patients; however, the following suggested dosage table is based on published clinical experience.
Total daily dosage should be divided and equal doses administered orally every 6 hours or at intervals according to individual patient needs. Disopyramide plasma levels and therapeutic response must be monitored closely. Patients should be hospitalized during the initial treatment period, and dose titration should start at the lower end of the ranges provided below.
| Age (years) | Disopyramide (mg/kg body weight/day) |
|---|---|
| Under 1 | 10 to 30 |
| 1 to 4 | 10 to 20 |
| 4 to 12 | 10 to 15 |
| 12 to 18 | 6 to 15 |
Since disopyramide phosphate 100 mg capsules contain 100 mg of disopyramide base, the pharmacist can readily prepare a 1 mg/mL to 10 mg/mL liquid suspension by adding the entire contents of disopyramide phosphate capsules to cherry syrup, (Prepare cherry syrup as follows: cherry juice, 475 mL; sucrose 800 g; alcohol, 20 mL; purified water, a sufficient quantity to make 1000 mL). The resulting suspension, when refrigerated, is stable for one month and should be thoroughly shaken before measurement of each dose. The suspension should be dispensed in an amber glass bottle with a child-resistant closure.
CONTRAINDICATIONS
Disopyramide phosphate capsules are contraindicated in the presence of cardiogenic shock, preexisting second- or third-degree AV block (if no pacemaker is present), congenital Q-T prolongation, or known hypersensitivity to the drug.
ADVERSE REACTIONS
The adverse reactions which were reported in disopyramide phosphate clinical trials encompass observations in 1,500 patients, including 90 patients studied for at least 4 years. The most serious adverse reactions are hypotension and congestive heart failure. The most common adverse reactions, which are dose dependent, are associated with the anticholinergic properties of the drug. These may be transitory, but may be persistent or can be severe. Urinary retention is the most serious anticholinergic effect.
The following reactions were reported in 10% to 40% of patients:
Anticholinergic: dry mouth (32%), urinary hesitancy (14%), constipation (11%)
The following reactions were reported in 3% to 9% of patients:
Anticholinergic: blurred vision, dry nose/eyes/throat
Genitourinary: urinary retention, urinary frequency and urgency
Gastrointestinal: nausea, pain/bloating/gas
General: dizziness, general fatigue/muscle weakness, headache, malaise, aches/pains
The following reactions were reported in 1% to 3% of patients:
Genitourinary: impotence
Cardiovascular: hypotension with or without congestive heart failure, increased congestive heart failure (see WARNINGS ), cardiac conduction disturbances (see WARNINGS ), edema/weight gain, shortness of breath, syncope, chest pain
Gastrointestinal: anorexia, diarrhea, vomiting
Dermatologic: generalized rash/dermatoses, itching
Central nervous system: nervousness
Other: hypokalemia, elevated cholesterol/triglycerides
The following reactions were reported in less than 1%:
Depression, insomnia, dysuria, numbness/tingling, elevated liver enzymes, AV block, elevated BUN, elevated creatinine, decreased hemoglobin/hematocrit
Hypoglycemia has been reported in association with disopyramide administration (see WARNINGS ).
Infrequent occurrences of reversible cholestatic jaundice, fever, and respiratory difficulty have been reported in association with disopyramide therapy, as have rare instances of thrombocytopenia, reversible agranulocytosis, and gynecomastia. Some cases of LE (lupus erythematosus) symptoms have been reported; most cases occurred in patients who had been switched to disopyramide from procainamide following the development of LE symptoms. Rarely, acute psychosis has been reported following disopyramide therapy, with prompt return to normal mental status when therapy was stopped. The physician should be aware of these possible reactions and should discontinue disopyramide phosphate therapy promptly if they occur.
To report SUSPECTED ADVERSE EVENTS, contact Mayne Pharma at 1-844-825-8500 or FDA at 1-800-FDA-1088 or http://www.fda.gov/ for voluntary reporting of adverse reactions.
Drug Interactions
If phenytoin or other hepatic enzyme inducers are taken concurrently with disopyramide, lower plasma levels of disopyramide may occur. Monitoring of disopyramide plasma levels is recommended in such concurrent use to avoid ineffective therapy. Other antiarrhythmic drugs (e.g., quinidine, procainamide, lidocaine, propranolol) have occasionally been used concurrently with disopyramide. Excessive widening of the QRS complex and/or prolongation of the Q-T interval may occur in these situations (see WARNINGS ). In healthy subjects, no significant drug-drug interaction was observed when disopyramide was coadministered with either propranolol or diazepam. Concomitant administration of disopyramide and quinidine resulted in slight increases in plasma disopyramide levels and slight decreases in plasma quinidine levels. Disopyramide does not increase serum digoxin levels.
Until data on possible interactions between verapamil and disopyramide phosphate are obtained, disopyramide should not be administered within 48 hours before or 24 hours after verapamil administration.
Although potent inhibitors of CYP3A4 (e.g., ketoconazole) have not been studied clinically, in vitro studies have shown that erythromycin and oleandomycin inhibit the metabolism of disopyramide. Cases of life-threatening interactions have been reported for disopyramide when given with clarithromycin and erythromycin indicating that co-administration of disopyramide with inhibitors of CYP3A4 could result in potentially fatal interaction.
DESCRIPTION
Disopyramide phosphate is an antiarrhythmic drug available for oral administration in immediate-release capsules containing 100 mg or 150 mg of disopyramide base, present as the phosphate. The base content of the phosphate salt is 77.6%. The structural formula of disopyramide phosphate is:
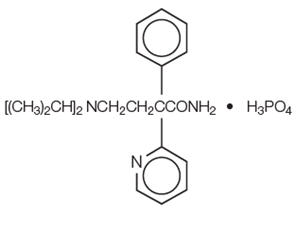 | ||
| C 21 H 29 N 3 O∙H 3 PO 4 | M.W. 437.47 | |
(±)-α-[2-(Diisopropylamino)ethyl]-α-phenyl-2-pyridineacetamide phosphate (1:1).
Disopyramide phosphate is freely soluble in water, and the free base (pKa 10.4) has an aqueous solubility of 1 mg/mL. The chloroform: water partition coefficient of the base is 3.1 at pH 7.2.
Disopyramide phosphate is a racemic mixture of d - and l -isomers. This drug is not chemically related to other antiarrhythmic drugs.
Disopyramide phosphate capsules (equivalent to 100 mg Disopyramide Base) and Disopyramide phosphate capsules (equivalent to 150 mg Disopyramide Base) contain the following inactive ingredients: magnesium stearate, microcrystalline cellulose and sodium lauryl sulfate. The capsule shells contain gelatin, methylparaben, propylparaben, and titanium dioxide.
The 100 mg capsule shell also contains D&C Red No. 28, D&C Yellow No. 10, FD&C Blue No. 1 and FD&C Red No. 40.
The 150 mg capsule shell also contains black iron oxide and red iron oxide.
CLINICAL PHARMACOLOGY
Mechanisms of Action
Disopyramide phosphate is a Type 1 antiarrhythmic drug (i.e., similar to procainamide and quinidine). In animal studies disopyramide decreases the rate of diastolic depolarization (phase 4) in cells with augmented automaticity, decreases the upstroke velocity (phase 0) and increases the action potential duration of normal cardiac cells, decreases the disparity in refractoriness between infarcted and adjacent normally perfused myocardium, and has no effect on alpha- or beta-adrenergic receptors.
Electrophysiology
In man, disopyramide at therapeutic plasma levels shortens the sinus node recovery time, lengthens the effective refractory period of the atrium, and has a minimal effect on the effective refractory period of the AV node. Little effect has been shown on AV-nodal and His-Purkinje conduction times or QRS duration. However, prolongation of conduction in accessory pathways occurs.
Hemodynamics
At recommended oral doses, disopyramide rarely produces significant alterations of blood pressure in patients without congestive heart failure (see WARNINGS ). With intravenous disopyramide, either increases in systolic/diastolic or decreases in systolic blood pressure have been reported, depending on the infusion rate and the patient population. Intravenous disopyramide may cause cardiac depression with an approximate mean 10% reduction of cardiac output, which is more pronounced in patients with cardiac dysfunction.
Anticholinergic Activity
The in vitro anticholinergic activity of disopyramide is approximately 0.06% that of atropine; however, the usual dose for disopyramide (as the phosphate) is 150 mg every 6 hours, compared to 0.4 to 0.6 mg for atropine (see WARNINGS and ADVERSE REACTIONS for anticholinergic side effects).
Pharmacokinetics
Following oral administration of immediate-release disopyramide phosphate, disopyramide phosphate is rapidly and almost completely absorbed, and peak plasma levels are usually attained within 2 hours. The usual therapeutic plasma levels of disopyramide base are 2 to 4 mcg/mL, and at these concentrations protein binding varies from 50% to 65%. Because of concentration-dependent protein binding, it is difficult to predict the concentration of the free drug when total drug is measured.
The mean plasma half-life of disopyramide in healthy humans is 6.7 hours (range of 4 to 10 hours). In six patients with impaired renal function (creatinine clearance less than 40 mL/min), disopyramide half-life values were 8 to 18 hours.
After the oral administration of 200 mg of disopyramide to 10 cardiac patients with borderline to moderate heart failure, the time to peak serum concentration of 2.3 ± 1.5 hours (mean ± SD) was increased, and the mean peak serum concentration of 4.8 ± 1.6 mcg/mL was higher than in healthy volunteers. After intravenous administration in these same patients, the mean elimination half-life was 9.7 ± 4.2 hours (range in healthy volunteers of 4.4 to 7.8 hours). In a second study of the oral administration of disopyramide to 7 patients with heart disease, including left ventricular dysfunction, the mean plasma half-life was slightly prolonged to 7.8 ± 1.9 hours (range of 5 to 9.5 hours).
In healthy men, about 50% of a given dose of disopyramide is excreted in the urine as the unchanged drug, about 20% as the mono-N-dealkylated metabolite, and 10% as the other metabolites. The plasma concentration of the major metabolite is approximately one tenth that of disopyramide. Altering the urinary pH in man does not affect the plasma half-life of disopyramide.
Drug Interactions
Effects of other drugs on disopyramide pharmacokinetics: In vitro metabolic studies indicated that disopyramide is metabolized by CYP3A4 and that inhibitors of this enzyme may result in elevation of plasma levels of disopyramide. Although specific drug interaction studies have not been done, cases of life-threatening interactions have been reported for disopyramide when given with clarithromycin and erythromycin.
HOW SUPPLIED
Disopyramide Phosphate Capsules (equivalent to 100 mg disopyramide base) are opaque orange capsules imprinted with m on one side and 095 on the other. Supplied in bottles of 100.
Disopyramide Phosphate Capsules (equivalent to 150 mg disopyramide base) are opaque brown capsules imprinted with m on one side and 096 on the other. Supplied in bottles of 100.
Dispense in a well-closed container with child-resistant closure.
Store at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature].
Mechanisms of Action
Disopyramide phosphate is a Type 1 antiarrhythmic drug (i.e., similar to procainamide and quinidine). In animal studies disopyramide decreases the rate of diastolic depolarization (phase 4) in cells with augmented automaticity, decreases the upstroke velocity (phase 0) and increases the action potential duration of normal cardiac cells, decreases the disparity in refractoriness between infarcted and adjacent normally perfused myocardium, and has no effect on alpha- or beta-adrenergic receptors.