Get your patient on Enalapril Maleate And Hydrochlorothiazide - Enalapril Maleate And Hydrochlorothiazide tablet (Enalapril Maleate And Hydrochlorothiazide)
Enalapril Maleate And Hydrochlorothiazide - Enalapril Maleate And Hydrochlorothiazide tablet prescribing information
USE IN PREGNANCY
When used in pregnancy during the second and third trimesters, ACE inhibitors can cause injury and even death to the developing fetus. When pregnancy is detected, enalapril maleate and hydrochlorothiazide tablets should be discontinued as soon as possible. See WARNINGS, Pregnancy, Enalapril Maleate, Fetal/Neonatal Morbidity and Mortality.
INDICATIONS AND USAGE
Enalapril maleate and hydrochlorothiazide tablets are indicated for the treatment of hypertension.
These fixed dose combinations are not indicated for initial treatment (see DOSAGE AND ADMINISTRATION ).
In using enalapril maleate and hydrochlorothiazide tablets, consideration should be given to the fact that another angiotensin converting enzyme inhibitor, captopril, has caused agranulocytosis, particularly in patients with renal impairment or collagen vascular disease, and that available data are insufficient to show that enalapril does not have a similar risk (see WARNINGS ).
In considering use of Enalapril maleate and hydrochlorothiazide tablets, it should be noted that black patients receiving ACE inhibitors have been reported to have a higher incidence of angioedema compared to non-blacks (see WARNINGS, Head and Neck Angioedema ).
DOSAGE AND ADMINISTRATION
Enalapril and hydrochlorothiazide are effective treatments for hypertension. The usual dosage range of enalapril is 10 to 40 mg per day administered in a single or two divided doses; hydrochlorothiazide is effective in doses of 12.5 to 50 mg daily. The side effects (see WARNINGS ) of enalapril are generally rare and apparently independent of dose; those of hydrochlorothiazide are a mixture of dose-dependent phenomena (primarily hypokalemia) and dose-independent phenomena (e.g., pancreatitis), the former much more common than the latter. Therapy with any combination of enalapril and hydrochlorothiazide will be associated with both sets of dose-independent side effects but the addition of enalapril in clinical trials blunted the hypokalemia normally seen with diuretics.
To minimize dose-independent side effects, it is usually appropriate to begin combination therapy only after a patient has failed to achieve the desired effect with monotherapy.
Dose Titration Guided by Clinical Effect
A patient whose blood pressure is not adequately controlled with either enalapril or hydrochlorothiazide monotherapy may be given enalapril maleate and hydrochlorothiazide tablets 5 mg/12.5 mg or enalapril maleate and hydrochlorothiazide tablets 10 mg/25 mg. Further increases of enalapril, hydrochlorothiazide or both depend on clinical response. The hydrochlorothiazide dose should generally not be increased until 2-3 weeks have elapsed. In general, patients do not require doses in excess of 20 mg of enalapril or 50 mg of hydrochlorothiazide. The daily dosage should not exceed four tablets of enalapril maleate and hydrochlorothiazide tablets 5 mg/12.5 mg or two tablets of enalapril maleate and hydrochlorothiazide tablets 10 mg/25 mg.
Replacement Therapy
The combination may be substituted for the titrated components.
Use in Renal Impairment
The usual regimens of therapy with enalapril maleate and hydrochlorothiazide tablets need not be adjusted as long as the patient's creatinine clearance is >30 mL/min/1.73m 2 (serum creatinine approximately ≤3 mg/dL or 265 µmol/L). In patients with more severe renal impairment, loop diuretics are preferred to thiazides, so enalapril maleate– hydrochlorothiazide is not recommended (see WARNINGS, Anaphylactoid reactions during membrane exposure ).
CONTRAINDICATIONS
Enalapril maleate and hydrochlorothiazide tablets are contraindicated in patients who are hypersensitive to any component of this product and in patients with a history of angioedema related to previous treatment with an angiotensin converting enzyme inhibitor and in patients with hereditary or idiopathic angioedema. Because of the hydrochlorothiazide component, this product is contraindicated in patients with anuria or hypersensitivity to other sulfonamide-derived drugs.
ADVERSE REACTIONS
Enalapril maleate and hydrochlorothiazide tablets has been evaluated for safety in more than 1500 patients, including over 300 patients treated for one year or more. In clinical trials with enalapril maleate and hydrochlorothiazide tablets no adverse experiences peculiar to this combination drug have been observed. Adverse experiences that have occurred, have been limited to those that have been previously reported with enalapril or hydrochlorothiazide.
The most frequent clinical adverse experiences in controlled trials were: dizziness (8.6 percent), headache (5.5 percent), fatigue (3.9 percent) and cough (3.5 percent). Generally, adverse experiences were mild and transient in nature. Adverse experiences occurring in greater than two percent of patients treated with enalapril maleate and hydrochlorothiazide tablets in controlled clinical trials are shown below.
| Percent of Patients in Controlled Studies | ||
|---|---|---|
| Enalapril maleate and hydrochlorothiazide tablets (n = 1580) Incidence (discontinuation) | Placebo (n=230) Incidence | |
| Dizziness | 8.6 (0.7) | 4.3 |
| Headache | 5.5 (0.4) | 9.1 |
| Fatigue | 3.9 (0.8) | 2.6 |
| Cough | 3.5 (0.4) | 0.9 |
| Muscle Cramps | 2.7 (0.2) | 0.9 |
| Nausea | 2.5 (0.4) | 1.7 |
| Asthenia | 2.4 (0.3) | 0.9 |
| Orthostatic Effects | 2.3 (<0.1) | 0.0 |
| Impotence | 2.2 (0.5) | 0.5 |
| Diarrhea | 2.1 (<0.1) | 1.7 |
Clinical adverse experiences occurring in 0.5 to 2.0 percent of patients in controlled trials included: Body As A Whole: Syncope, chest pain, abdominal pain; Cardiovascular: Orthostatic hypotension, palpitation, tachycardia; Digestive: Vomiting, dyspepsia, constipation, flatulence, dry mouth; Nervous/Psychiatric: Insomnia, nervousness, paresthesia, somnolence, vertigo; Skin: Pruritus, rash; Other: Dyspnea, gout, back pain, arthralgia, diaphoresis, decreased libido, tinnitus, urinary tract infection.
Angioedema
Angioedema has been reported in patients receiving enalapril maleate and hydrochlorothiazide tablets, with an incidence higher in black than in non-black patients. Angioedema associated with laryngeal edema may be fatal. If angioedema of the face, extremities, lips, tongue, glottis and/or larynx occurs, treatment with enalapril maleate and hydrochlorothiazide tablets should be discontinued and appropriate therapy instituted immediately (see WARNINGS ).
Hypotension
In clinical trials, adverse effects relating to hypotension occurred as follows: hypotension (0.9 percent), orthostatic hypotension (1.5 percent), other orthostatic effects (2.3 percent). In addition syncope occurred in 1.3 percent of patients (see WARNINGS ).
Cough
See PRECAUTIONS, Cough .
Clinical Laboratory Test Findings
Serum Electrolytes
See PRECAUTIONS .
Creatinine, Blood Urea Nitrogen
In controlled clinical trials minor increases in blood urea nitrogen and serum creatinine, reversible upon discontinuation of therapy, were observed in about 0.6 percent of patients with essential hypertension treated with enalapril maleate and hydrochlorothiazide tablets. More marked increases have been reported in other enalapril experience. Increases are more likely to occur in patients with renal artery stenosis (see PRECAUTIONS ).
Serum Uric Acid, Glucose, Magnesium, and Calcium
See PRECAUTIONS .
Hemoglobin and Hematocrit
Small decreases in hemoglobin and hematocrit (mean decreases of approximately 0.3 g percent and 1.0 vol percent, respectively) occur frequently in hypertensive patients treated with enalapril maleate and hydrochlorothiazide tablets but are rarely of clinical importance unless another cause of anemia coexists. In clinical trials, less than 0.1 percent of patients discontinued therapy due to anemia.
Liver Function Tests
Rarely, elevations of liver enzymes and/or serum bilirubin have occurred (see WARNINGS, Hepatic Failure ).
Other adverse reactions that have been reported with the individual components are listed below and, within each category, are in order of decreasing severity.
Enalapril Maleate
Enalapril has been evaluated for safety in more than 10,000 patients. In clinical trials adverse reactions which occurred with enalapril were also seen with enalapril maleate and hydrochlorothiazide tablets. However, since enalapril has been marketed, the following adverse reactions have been reported: Body As A Whole: Anaphylactoid reactions (see WARNINGS, Anaphylactoid reactions during membrane exposure ); Cardiovascular: Cardiac arrest; myocardial infarction or cerebrovascular accident, possibly secondary to excessive hypotension in high risk patients (see WARNINGS, Hypotension ); pulmonary embolism and infarction; pulmonary edema; rhythm disturbances including atrial tachycardia and bradycardia; atrial fibrillation; hypotension; angina pectoris, Raynaud's phenomenon; Digestive : Ileus, pancreatitis, hepatic failure, hepatitis (hepatocellular [proven on rechallenge] or cholestatic jaundice) (see WARNINGS, Hepatic Failure ), melena, anorexia, glossitis, stomatitis, dry mouth; Hematologic: Rare cases of neutropenia, thrombocytopenia and bone marrow depression. Hemolytic anemia, including cases of hemolysis in patients with G-6-PD deficiency, has been reported; a causal relationship to enalapril cannot be excluded. Nervous System/Psychiatric: Depression, confusion, ataxia, peripheral neuropathy (e.g., paresthesia, dysesthesia), dream abnormality; Urogenital: Renal failure, oliguria, renal dysfunction, (see PRECAUTIONS and DOSAGE AND ADMINISTRATION ), flank pain, gynecomastia; Respiratory: Pulmonary infiltrates, eosinophilic pneumonitis, bronchospasm, pneumonia, bronchitis, rhinorrhea, sore throat and hoarseness, asthma, upper respiratory infection; Skin: Exfoliative dermatitis, toxic epidermal necrolysis, Stevens-Johnson syndrome, herpes zoster, erythema multiforme, urticaria, pemphigus, alopecia, flushing, photosensitivity; Special Senses: Blurred vision, taste alteration, anosmia, conjunctivitis, dry eyes, tearing.
Miscellaneous
A symptom complex has been reported which may include some or all of the following: a positive ANA, an elevated erythrocyte sedimentation rate, arthralgia/arthritis, myalgia/myositis, fever, serositis, vasculitis, leukocytosis, eosinophilia, photosensitivity, rash and other dermatologic manifestations.
Fetal/Neonatal Morbidity and Mortality
Hydrochlorothiazide
Body as a Whole: Weakness; Digestive: Pancreatitis, jaundice (intrahepatic cholestatic jaundice), sialadenitis, cramping, gastric irritation, anorexia; Hematologic: Aplastic anemia, agranulocytosis, leukopenia, hemolytic anemia, thrombocytopenia; Hypersensitivity: Purpura, photosensitivity, urticaria, necrotizing angiitis (vasculitis and cutaneous vasculitis), fever, respiratory distress including pneumonitis and pulmonary edema, anaphylactic reactions; Musculoskeletal: Muscle spasm; Nervous System/Psychiatric: Restlessness; Renal: Renal failure, renal dysfunction, interstitial nephritis (see WARNINGS ); Skin: Erythema multiforme including Stevens-Johnson syndrome, exfoliative dermatitis including toxic epidermal necrolysis, alopecia; Special Senses: Transient blurred vision, xanthopsia.
Drug Interactions
Enalapril Maleate
Hypotension ? Patients on Diuretic Therapy
Patients on diuretics and especially those in whom diuretic therapy was recently instituted, may occasionally experience an excessive reduction of blood pressure after initiation of therapy with enalapril. The possibility of hypotensive effects with enalapril can be minimized by either discontinuing the diuretic or increasing the salt intake prior to initiation of treatment with enalapril. If it is necessary to continue the diuretic, provide medical supervision for at least two hours and until blood pressure has stabilized for at least an additional hour (see WARNINGS , and DOSAGE AND ADMINISTRATION ).
Agents Causing Renin Release
The antihypertensive effect of enalapril is augmented by antihypertensive agents that cause rennin release (e.g., diuretics).
Non-steroidal Anti-inflammatory Agents
In some patients with compromised renal function who are being treated with nonsteroidal anti-inflammatory drugs, the coadministration of enalapril may result in a further deterioration of renal function. These effects are usually reversible.
In a clinical pharmacology study, indomethacin or sulindac was administered to hypertensive patients receiving enalapril maleate. In this study there was no evidence of a blunting of the antihypertensive action of enalapril maleate. However, reports suggest that NSAIDs may diminish the antihypertensive effect of ACE inhibitors. This interaction should be given consideration in patients taking NSAIDs concomitantly with ACE inhibitors.
Other Cardiovascular Agents
Enalapril has been used concomitantly with beta adrenergic-blocking agents, methyldopa, nitrates, calcium-blocking agents, hydralazine and prazosin without evidence of clinically significant adverse interactions.
Agents Increasing Serum Potassium
Enalapril attenuates diuretic-induced potassium loss. Potassium-sparing diuretics (e.g., spironolactone, triamterene, or amiloride), potassium supplements, or potassium-containing salt substitutes may lead to significant increases in serum potassium. Therefore, if concomitant use of these agents is indicated because of demonstrated hypokalemia they should be used with caution and with frequent monitoring of serum potassium.
Lithium
Lithium toxicity has been reported in patients receiving lithium concomitantly with drugs which cause elimination of sodium, including ACE inhibitors. A few cases of lithium toxicity have been reported in patients receiving concomitant enalapril and lithium and were reversible upon discontinuation of both drugs. It is recommended that serum lithium levels be monitored frequently if enalapril is administered concomitantly with lithium.
Gold
Nitritoid reactions (symptoms include facial flushing, nausea, vomiting and hypotension) have been reported rarely in patients on therapy with injectable gold (sodium aurothiomalate) and concomitant ACE Inhibitor therapy including enalapril maleate and hydrochlorothiazide.
Hydrochlorothiazide
When administered concurrently the following drugs may interact with thiazide diuretics:
Alcohol, Barbiturates, or Narcotics — potentiation of orthostatic hypotension may occur.
Antidiabetic Drugs (Oral Agents and Insulin) — dosage adjustment of the antidiabetic drug may be required.
Other Antihypertensive Drugs — additive effect or potentiation.
Cholestyramine and Colestipol Resins — Absorption of hydrochlorothiazide is impaired in the presence of anionic exchange resins. Single doses of either cholestyramine or colestipol resins bind the hydrochlorothiazide and reduce its absorption from the gastrointestinal tract by up to 85 and 43 percent, respectively.
Corticosteroids, ACTH — intensified electrolyte depletion, particularly hypokalemia.
Pressor Amines (e.g., Norepinephrine) — possible decreased response to pressor amines but not sufficient to preclude their use.
Skeletal Muscle Relaxants, Nondepolarizing (e.g., Tubocurarine) — possible increased responsiveness to the muscle relaxant.
Lithium — should not generally be given with diuretics. Diuretic agents reduce the renal clearance of lithium and add a high risk of lithium toxicity. Refer to the package insert for lithium preparations before use of such preparations with enalapril maleate and hydrochlorothiazide tablets.
Non-steroidal Anti-inflammatory Drugs — In some patients, the administration of a non-steroidal anti-inflammatory agent can reduce the diuretic, natriuretic, and antihypertensive effects of loop, potassium-sparing and thiazide diuretics. Therefore, when enalapril maleate and hydrochlorothiazide tablets and non-steroidal anti-inflammatory agents are used concomitantly, the patient should be observed closely to determine if the desired effect of the diuretic is obtained.
DESCRIPTION
Enalapril maleate-hydrochlorothiazide combines an angiotensin converting enzyme inhibitor, enalapril maleate, and a diuretic, hydrochlorothiazide.
Enalapril maleate is the maleate salt of enalapril, the ethyl ester of a long-acting angiotensin converting enzyme inhibitor, enalaprilat. Enalapril maleate is chemically described as ( S )-1-[ N -[1-(ethoxycarbonyl ) -3- phenylpropyl]-L-alanyl]-L-proline, (Z)-2-butenedioate salt (1:1).
Its molecular formula is C 20 H 28 N 2 O 5 • C 4 H 4 O 4 , and its structural formula is:
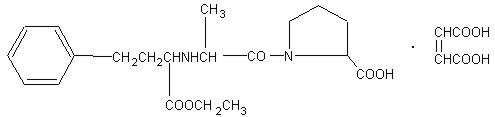
Enalapril maleate is a white to off-white crystalline powder with a molecular weight of 492.53. It is sparingly soluble in water, soluble in ethanol, and freely soluble in methanol.
Enalapril is a pro-drug; following oral administration, it is bioactivated by hydrolysis of the ethyl ester to enalaprilat, which is the active angiotensin converting enzyme inhibitor.
Hydrochlorothiazide is 6-chloro-3,4-dihydro-2 H -1,2,4-benzothiadiazine-7-sulfonamide 1,1-dioxide. Its molecular formula is C 7 H 8 ClN 3 O 4 S 2 , and its structural formula is:
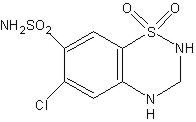
It is a white, or practically white, crystalline powder with a molecular weight of 297.74, which is slightly soluble in water, but freely soluble in sodium hydroxide solution.
Enalapril maleate and hydrochlorothiazide tablets are available in two tablet combinations of enalapril maleate with hydrochlorothiazide: Enalapril maleate and hydrochlorothiazide tablets 5 mg/12.5 mg, containing 5 mg enalapril maleate and 12.5 mg hydrochlorothiazide and Enalapril maleate and hydrochlorothiazide tablets 10 mg/25 mg, containing 10 mg enalapril maleate and 25 mg hydrochlorothiazide. Inactive ingredients are: lactose monohydrate, pregelatinized starch, starch (corn starch), zinc stearate, and purified water.
CLINICAL PHARMACOLOGY
As a result of its diuretic effects, hydrochlorothiazide increases plasma renin activity, increases aldosterone secretion, and decreases serum potassium. Administration of enalapril maleate blocks the renin-angiotensin-aldosterone axis and tends to reverse the potassium loss associated with the diuretic.
In clinical studies, the extent of blood pressure reduction seen with the combination of enalapril maleate and hydrochlorothiazide was approximately additive. The antihypertensive effect of enalapril maleate and hydrochlorothiazide tablets was usually sustained for at least 24 hours.
Concomitant administration of enalapril maleate and hydrochlorothiazide has little, or no effect on the bioavailability of either drug. The combination tablet is bioequivalent to concomitant administration of the separate entities.
Enalapril Maleate
Mechanism of Action
Enalapril, after hydrolysis to enalaprilat, inhibits angiotensin-converting enzyme (ACE) in human subjects and animals. ACE is a peptidyl dipeptidase that catalyzes the conversion of angiotensin I to the vasoconstrictor substance, angiotensin II. Angiotensin II also stimulates aldosterone secretion by the adrenal cortex. Inhibition of ACE results in decreased plasma angiotensin II, which leads to decreased vasopressor activity and to decreased aldosterone secretion. Although the latter decrease is small, it results in small increases of serum potassium. In hypertensive patients treated with enalapril maleate alone for up to 48 weeks, mean increases in serum potassium of approximately 0.2 mEq/L were observed. In patients treated with enalapril maleate plus a thiazide diuretic, there was essentially no change in serum potassium (see PRECAUTIONS ). Removal of angiotensin II negative feedback on rennin secretion leads to increased plasma renin activity.
ACE is identical to kininase, an enzyme that degrades bradykinin. Whether increased levels of bradykinin, a potent vasodepressor peptide, play a role in the therapeutic effects of enalapril remains to be elucidated.
While the mechanism through which enalapril lowers blood pressure is believed to be primarily suppression of the renin-angiotensin-aldosterone system, enalapril is antihypertensive even in patients with low-renin hypertension. Although enalapril was antihypertensive in all races studied, black hypertensive patients (usually a low-renin hypertensive population) had a smaller average response to enalapril maleate monotherapy than non-black patients. In contrast, hydrochlorothiazide was more effective in black patients than enalapril. Concomitant administration of enalapril maleate and hydrochlorothiazide was equally effective in black and non-black patients.
Pharmacokinetics and Metabolism
Following oral administration of enalapril maleate, peak serum concentrations of enalapril occur within about one hour. Based on urinary recovery, the extent of absorption of enalapril is approximately 60 percent. Enalapril absorption is not influenced by the presence of food in the gastrointestinal tract. Following absorption, enalapril is hydrolyzed to enalaprilat, which is a more potent angiotensin converting enzyme inhibitor than enalapril; enalaprilat is poorly absorbed when administered orally. Peak serum concentrations of enalaprilat occur three to four hours after an oral dose of enalapril maleate. Excretion of enalaprilat and enalapril is primarily renal. Approximately 94 percent of the dose is recovered in the urine and feces as enalaprilat or enalapril. The principal components in urine are enalaprilat, accounting for about 40 percent of the dose, and intact enalapril. There is no evidence of metabolites of enalapril, other than enalaprilat.
The serum concentration profile of enalaprilat exhibits a prolonged terminal phase, apparently representing a small fraction of the administered dose that has been bound to ACE. The amount bound does not increase with dose, indicating a saturable site of binding. The effective half-life for accumulation of enalaprilat following multiple doses of enalapril maleate is 11 hours.
The disposition of enalapril and enalaprilat in patients with renal insufficiency is similar to that in patients with normal renal function until the glomerular filtration rate is 30 mL/min or less. With glomerular filtration rate ≤ 30 mL/min, peak and trough enalaprilat levels increase, time to peak concentration increases and time to steady state may be delayed. The effective half-life of enalaprilat following multiple doses of enalapril maleate is prolonged at this level of renal insufficiency. Enalaprilat is dialyzable at the rate of 62 mL/min.
Studies in dogs indicate that enalapril crosses the blood-brain barrier poorly, if at all; enalaprilat does not enter the brain. Multiple doses of enalapril maleate in rats do not result in accumulation in any tissues. Milk of lactating rats contains radioactivity following administration of 14 C enalapril maleate. Radioactivity was found to cross the placenta following administration of labeled drug to pregnant hamsters.
Pharmacodynamics
Administration of enalapril maleate to patients with hypertension of severity ranging from mild to severe results in a reduction of both supine and standing blood pressure usually with no orthostatic component. Symptomatic postural hypotension is infrequent with enalapril alone but it can be anticipated in volume-depleted patients, such as patients treated with diuretics. In clinical trials with enalapril and hydrochlorothiazide administered concurrently, syncope occurred in 1.3 percent of patients (see WARNINGS and DOSAGE AND ADMINISTRATION ).
In most patients studied, after oral administration of a single dose of enalapril maleate, onset of antihypertensive activity was seen at one hour with peak reduction of blood pressure achieved by four to six hours.
At recommended doses, antihypertensive effects of enalapril maleate monotherapy have been maintained for at least 24 hours. In some patients the effects may diminish toward the end of the dosing interval; this was less frequently observed with concomitant administration of enalapril maleate and hydrochlorothiazide.
Achievement of optimal blood pressure reduction may require several weeks of enalapril therapy in some patients.
The antihypertensive effects of enalapril have continued during long term therapy. Abrupt withdrawal of enalapril has not been associated with a rapid increase in blood pressure.
In hemodynamic studies in patients with essential hypertension, blood pressure reduction produced by enalapril was accompanied by a reduction in peripheral arterial resistance with an increase in cardiac output and little or no change in heart rate. Following administration of enalapril maleate, there is an increase in renal blood flow; glomerular filtration rate is usually unchanged. The effects appear to be similar in patients with renovascular hypertension.
In a clinical pharmacology study, indomethacin or sulindac was administered to hypertensive patients receiving enalapril maleate. In this study there was no evidence of a blunting of the antihypertensive action of enalapril maleate (see PRECAUTIONS, Drug Interactions, Enalapril maleate ).
Hydrochlorothiazide
The mechanism of the antihypertensive effect of thiazides is unknown. Thiazides do not usually affect normal blood pressure. Hydrochlorothiazide is a diuretic and antihypertensive. It affects the distal renal tubular mechanism of electrolyte reabsorption.
Hydrochlorothiazide increases excretion of sodium and chloride in approximately equivalent amounts. Natriuresis may be accompanied by some loss of potassium and bicarbonate. After oral use diuresis begins within two hours, peaks in about four hours and lasts about 6 to 12 hours. Hydrochlorothiazide is not metabolized but is eliminated rapidly by the kidney. When plasma levels have been followed for at least 24 hours, the plasma half-life has been observed to vary between 5.6 and 14.8 hours. At least 61 percent of the oral dose is eliminated unchanged within 24 hours. Hydrochlorothiazide crosses the placental but not the blood-brain barrier.
HOW SUPPLIED
Enalapril maleate and hydrochlorothiazide tablets USP, 5 mg/12.5 mg are white, round, flat compressed tablets with beveled edge, embossed “ C ” 133 on one side and plain on other side and are supplied in bottles of 100’s and 1000’s.
Bottles of 100 (with desiccant) NDC 55111-133-01. Bottles of 1000 (with desiccant) NDC 55111-133-10.
Enalapril maleate and hydrochlorothiazide tablets USP, 10 mg/25 mg are white, round, flat compressed tablets with beveled edge, embossed “ C ” 134 on one side and plain on other side and are supplied in bottles of 100’s and 1000’s.
Bottles of 100 (with desiccant) NDC 55111-134-01. Bottles of 1000 (with desiccant) NDC 55111-134-10.
Storage
Store at 20°– 25°C (68°–77°F); [See USP Controlled Room Temperature]. Keep container tightly closed. Protect from moisture.Dispense in a tight container as per USP, if product package is subdivided.
Mechanism of Action
Enalapril, after hydrolysis to enalaprilat, inhibits angiotensin-converting enzyme (ACE) in human subjects and animals. ACE is a peptidyl dipeptidase that catalyzes the conversion of angiotensin I to the vasoconstrictor substance, angiotensin II. Angiotensin II also stimulates aldosterone secretion by the adrenal cortex. Inhibition of ACE results in decreased plasma angiotensin II, which leads to decreased vasopressor activity and to decreased aldosterone secretion. Although the latter decrease is small, it results in small increases of serum potassium. In hypertensive patients treated with enalapril maleate alone for up to 48 weeks, mean increases in serum potassium of approximately 0.2 mEq/L were observed. In patients treated with enalapril maleate plus a thiazide diuretic, there was essentially no change in serum potassium (see PRECAUTIONS ). Removal of angiotensin II negative feedback on rennin secretion leads to increased plasma renin activity.
ACE is identical to kininase, an enzyme that degrades bradykinin. Whether increased levels of bradykinin, a potent vasodepressor peptide, play a role in the therapeutic effects of enalapril remains to be elucidated.
While the mechanism through which enalapril lowers blood pressure is believed to be primarily suppression of the renin-angiotensin-aldosterone system, enalapril is antihypertensive even in patients with low-renin hypertension. Although enalapril was antihypertensive in all races studied, black hypertensive patients (usually a low-renin hypertensive population) had a smaller average response to enalapril maleate monotherapy than non-black patients. In contrast, hydrochlorothiazide was more effective in black patients than enalapril. Concomitant administration of enalapril maleate and hydrochlorothiazide was equally effective in black and non-black patients.