Get your patient on Flumazenil - Flumazenil injection, Solution (Flumazenil)
Flumazenil - Flumazenil injection, Solution prescribing information
INDICATIONS AND USAGE:
Adult Patients
Flumazenil Injection, USP is indicated for the complete or partial reversal of the sedative effects of benzodiazepines in cases where general anesthesia has been induced and/or maintained with benzodiazepines, where sedation has been produced with benzodiazepines for diagnostic and therapeutic procedures, and for the management of benzodiazepine overdose.
Pediatric Patients (aged 1 to 17)
Flumazenil Injection, USP is indicated for the reversal of conscious sedation induced with benzodiazepines (see PRECAUTIONS , Pediatric Use ).
DOSAGE AND ADMINISTRATION:
Flumazenil Injection, USP is recommended for intravenous use only. It is compatible with 5% dextrose in water, lactated Ringer’s and normal saline solutions. If Flumazenil Injection, USP is drawn into a syringe or mixed with any of these solutions, it should be discarded after 24 hours. For optimum sterility, Flumazenil Injection, USP should remain in the vial until just before use. As with all parenteral drug products, Flumazenil Injection, USP should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
To minimize the likelihood of pain at the injection site, Flumazenil Injection, USP should be administered through a freely running intravenous infusion into a large vein.
Reversal of Conscious Sedation
Adult Patients
For the reversal of the sedative effects of benzodiazepines administered for conscious sedation, the recommended initial dose of Flumazenil Injection, USP is 0.2 mg (2 mL) administered intravenously over 15 seconds. If the desired level of consciousness is not obtained after waiting an additional 45 seconds, a further dose of 0.2 mg (2 mL) can be injected and repeated at 60-second intervals where necessary (up to a maximum of 4 additional times) to a maximum total dose of 1 mg (10 mL). The dosage should be individualized based on the patient’s response, with most patients responding to doses of 0.6 mg to 1 mg (see Individualization of Dosage ).
In the event of resedation, repeated doses may be administered at 20-minute intervals as needed. For repeat treatment, no more than 1 mg (given as 0.2 mg/min) should be administered at any one time, and no more than 3 mg should be given in any one hour.
It is recommended that Flumazenil Injection, USP be administered as the series of small injections described (not as a single bolus injection) to allow the practitioner to control the reversal of sedation to the approximate endpoint desired and to minimize the possibility of adverse effects (see Individualization of Dosage ).
Pediatric Patients
For the reversal of the sedative effects of benzodiazepines administered for conscious sedation in pediatric patients greater than 1 year of age, the recommended initial dose is 0.01 mg/kg (up to 0.2 mg) administered intravenously over 15 seconds. If the desired level of consciousness is not obtained after waiting an additional 45 seconds, further injections of 0.01 mg/kg (up to 0.2 mg) can be administered and repeated at 60-second intervals where necessary (up to a maximum of 4 additional times) to a maximum total dose of 0.05 mg/kg or 1 mg, whichever is lower. The dose should be individualized based on the patient’s response. The mean total dose administered in the pediatric clinical trial of flumazenil was 0.65 mg (range: 0.08 mg to 1 mg). Approximately one-half of patients required the maximum of five injections.
Resedation occurred in 7 of 60 patients who were fully alert 10 minutes after the start of Flumazenil Injection, USP administration (see PRECAUTIONS, Pediatric Use ). The safety and efficacy of repeated flumazenil administration in pediatric patients experiencing resedation have not been established.
It is recommended that Flumazenil Injection, USP be administered as the series of small injections described (not as a single bolus injection) to allow the practitioner to control the reversal of sedation to the approximate endpoint desired and to minimize the possibility of adverse effects (see Individualization of Dosage ).
The safety and efficacy of Flumazenil Injection, USP in the reversal of conscious sedation in pediatric patients below the age of 1 year have not been established.
Reversal of General Anesthesia in Adult Patients
For the reversal of the sedative effects of benzodiazepines administered for general anesthesia, the recommended initial dose of Flumazenil Injection, USP is 0.2 mg (2 mL) administered intravenously over 15 seconds. If the desired level of consciousness is not obtained after waiting an additional 45 seconds, a further dose of 0.2 mg (2 mL) can be injected and repeated at 60-second intervals where necessary (up to a maximum of 4 additional times) to a maximum total dose of 1 mg (10 mL). The dosage should be individualized based on the patient’s response, with most patients responding to doses of 0.6 mg to 1 mg (see Individualization of Dosage ).
In the event of resedation, repeated doses may be administered at 20-minute intervals as needed. For repeat treatment, no more than 1 mg (given as 0.2 mg/min) should be administered at any one time, and no more than 3 mg should be given in any one hour.
It is recommended that Flumazenil Injection, USP be administered as the series of small injections described (not as a single bolus injection) to allow the practitioner to control the reversal of sedation to the approximate endpoint desired and to minimize the possibility of adverse effects (see Individualization of Dosage ).
Management of Suspected Benzodiazepine Overdose in Adult Patients
For initial management of a known or suspected benzodiazepine overdose, the recommended initial dose of Flumazenil Injection, USP is 0.2 mg (2 mL) administered intravenously over 30 seconds. If the desired level of consciousness is not obtained after waiting 30 seconds, a further dose of 0.3 mg (3 mL) can be administered over another 30 seconds. Further doses of 0.5 mg (5 mL) can be administered over 30 seconds at 1-minute intervals up to a cumulative dose of 3 mg.
Do not rush the administration of Flumazenil Injection, USP. Patients should have a secure airway and intravenous access before administration of the drug and be awakened gradually (see PRECAUTIONS ).
Most patients with a benzodiazepine overdose will respond to a cumulative dose of 1 mg to 3 mg of Flumazenil Injection, USP, and doses beyond 3 mg do not reliably produce additional effects. On rare occasions, patients with a partial response at 3 mg may require additional titration up to a total dose of 5 mg (administered slowly in the same manner).
If a patient has not responded 5 minutes after receiving a cumulative dose of 5 mg of Flumazenil Injection, USP, the major cause of sedation is likely not to be due to benzodiazepines, and additional Flumazenil Injection, USP is likely to have no effect.
In the event of resedation, repeated doses may be given at 20-minute intervals if needed. For repeat treatment, no more than 1 mg (given as 0.5 mg/min) should be given at any one time and no more than 3 mg should be given in any one hour.
Safety and Handling
Flumazenil Injection, USP is supplied in sealed dosage forms and poses no known risk to the healthcare provider. Routine care should be taken to avoid aerosol generation when preparing syringes for injection, and spilled medication should be rinsed from the skin with cool water.
CONTRAINDICATIONS:
Flumazenil Injection, USP is contraindicated:
• in patients with a known hypersensitivity to flumazenil or benzodiazepines.
• in patients who have been given a benzodiazepine for control of a potentially life-threatening condition (e.g., control of intracranial pressure or status epilepticus).
• in patients who are showing signs of serious cyclic antidepressant overdose (see WARNINGS ).
ADVERSE REACTIONS:
To report SUSPECTED ADVERSE REACTIONS, contact Fresenius Kabi USA, LLC, at 1-800-551-7176 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Serious Adverse Reactions
Deaths have occurred in patients who received flumazenil in a variety of clinical settings. The majority of deaths occurred in patients with serious underlying disease or in patients who had ingested large amounts of non-benzodiazepine drugs (usually cyclic antidepressants), as part of an overdose.
Serious adverse events have occurred in all clinical settings, and convulsions are the most common serious adverse events reported. Flumazenil administration has been associated with the onset of convulsions in patients with severe hepatic impairment and in patients who are relying on benzodiazepine effects to control seizures, are physically dependent on benzodiazepines, or who have ingested large doses of other drugs (mixed-drug overdose) (see WARNINGS ).
Two of the 446 patients who received flumazenil in controlled clinical trials for the management of a benzodiazepine overdose had cardiac dysrhythmias (1 ventricular tachycardia, 1 junctional tachycardia).
Adverse Events in Clinical Studies
The following adverse reactions were considered to be related to flumazenil administration (both alone and for the reversal of benzodiazepine effects) and were reported in studies involving 1875 individuals who received flumazenil in controlled trials. Adverse events most frequently associated with flumazenil alone were limited to dizziness, injection site pain, increased sweating, headache, and abnormal or blurred vision (3% to 9%).
Body as a Whole: fatigue (asthenia, malaise), headache, injection site pain• and injection site reaction (thrombophlebitis, skin abnormality, rash)
Cardiovascular System: cutaneous vasodilation (sweating, flushing, hot flushes)
Digestive System: nausea and vomiting (11%)
Nervous System: agitation (anxiety, nervousness, dry mouth, tremor, palpitations, insomnia, dyspnea, hyperventilation)•, dizziness (vertigo, ataxia) (10%) and emotional lability (crying abnormal, depersonalization, euphoria, increased tears, depression, dysphoria, paranoia)
Special Senses: abnormal vision (visual field defect, diplopia) and paresthesia (sensation abnormal, hypoesthesia)
All adverse reactions occurred in 1% to 3% of cases unless otherwise marked.
•indicates reaction in 3% to 9% of cases.
Observed percentage reported if greater than 9%.
The following adverse events were observed infrequently (less than 1%) in the clinical studies, but were judged as probably related to flumazenil administration and/or reversal of benzodiazepine effects:
Nervous System: confusion (difficulty concentrating, delirium), convulsions (see WARNINGS ) and somnolence (stupor)
Special Senses: abnormal hearing (transient hearing impairment, hyperacusis, tinnitus)
The following adverse events occurred with frequencies less than 1% in the clinical trials. Their relationship to flumazenil administration is unknown, but they are included as alerting information for the physician.
Body as a Whole: rigors, shivering
Cardiovascular System: arrhythmia (atrial, nodal, ventricular extrasystoles), bradycardia, tachycardia, hypertension and chest pain
Digestive System: hiccup
Nervous System: speech disorder (dysphonia, thick tongue)
Not included in this list is operative site pain that occurred with the same frequency in patients receiving placebo as in patients receiving flumazenil for reversal of sedation following a surgical procedure.
Additional Adverse Reactions Reported During Postmarketing Experience
The following events have been reported during postapproval use of flumazenil.
Nervous System: Fear, panic attacks in patients with a history of panic disorders.
Withdrawal symptoms may occur following rapid injection of flumazenil in patients with long-term exposure to benzodiazepines.
DESCRIPTION:
Flumazenil Injection, USP is a benzodiazepine receptor antagonist. Chemically, flumazenil is ethyl 8-fluoro-5,6-dihydro-5-methyl-6-oxo-4H-imidazo [1,5-a] (1,4) benzodiazepine-3-carboxylate. Flumazenil has an imidazobenzodiazepine structure and the following structural formula:
Flumazenil is a white to off-white crystalline compound with an octanol:buffer partition coefficient of 14 to 1 at pH 7.4. It is insoluble in water but slightly soluble in acidic aqueous solutions. Flumazenil Injection, USP is available as a sterile parenteral dosage form for intravenous administration. Each mL contains 0.1 mg of flumazenil compounded with 1.8 mg of methylparaben, 0.2 mg of propylparaben, 0.9% sodium chloride, 0.01% edetate disodium, and 0.01% acetic acid; the pH is adjusted to approximately 3.8 to 4.3 with hydrochloric acid and/or, if necessary, sodium hydroxide.
CLINICAL PHARMACOLOGY:
Flumazenil, an imidazobenzodiazepine derivative, antagonizes the actions of benzodiazepines on the central nervous system. Flumazenil competitively inhibits the activity at the benzodiazepine recognition site on the GABA/benzodiazepine receptor complex. Flumazenil is a weak partial agonist in some animal models of activity, but has little or no agonist activity in man.
Flumazenil does not antagonize the central nervous system effects of drugs affecting GABA-ergic neurons by means other than the benzodiazepine receptor (including ethanol, barbiturates, or general anesthetics) and does not reverse the effects of opioids.
In animals pretreated with high doses of benzodiazepines over several weeks, flumazenil elicited symptoms of benzodiazepine withdrawal, including seizures. A similar effect was seen in adult human subjects.
Pharmacodynamics
Intravenous flumazenil has been shown to antagonize sedation, impairment of recall, psychomotor impairment and ventilatory depression produced by benzodiazepines in healthy human volunteers.
The duration and degree of reversal of benzodiazepine effects are related to the dose and plasma concentrations of flumazenil as shown in the following data from a study in normal volunteers.
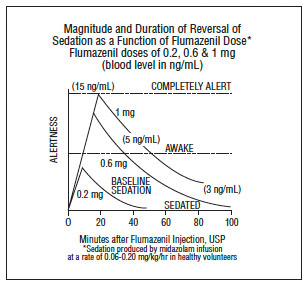
Generally, doses of approximately 0.1 mg to 0.2 mg (corresponding to peak plasma levels of 3 to 6 ng/mL) produce partial antagonism, whereas higher doses of 0.4 to 1 mg (peak plasma levels of 12 to 28 ng/mL) usually produce complete antagonism in patients who have received the usual sedating doses of benzodiazepines. The onset of reversal is usually evident within 1 to 2 minutes after the injection is completed. Eighty percent response will be reached within 3 minutes, with the peak effect occurring at 6 to 10 minutes. The duration and degree of reversal are related to the plasma concentration of the sedating benzodiazepine as well as the dose of flumazenil given.
In healthy volunteers, flumazenil did not alter intraocular pressure when given alone and reversed the decrease in intraocular pressure seen after administration of midazolam.
Pharmacokinetics
After IV administration, plasma concentrations of flumazenil follow a two-exponential decay model. The pharmacokinetics of flumazenil are dose-proportional up to 100 mg.
Distribution
Flumazenil is extensively distributed in the extravascular space with an initial distribution half-life of 4 to 11 minutes and a terminal half-life of 40 to 80 minutes. Peak concentrations of flumazenil are proportional to dose, with an apparent initial volume of distribution of 0.5 L/kg. The volume of distribution at steady-state is 0.9 to 1.1 L/kg. Flumazenil is a weak lipophilic base. Protein binding is approximately 50% and the drug shows no preferential partitioning into red blood cells. Albumin accounts for two thirds of plasma protein binding.
Metabolism
Flumazenil is completely (99%) metabolized. Very little unchanged flumazenil (<1%) is found in the urine. The major metabolites of flumazenil identified in urine are the de-ethylated free acid and its glucuronide conjugate. In preclinical studies there was no evidence of pharmacologic activity exhibited by the de-ethylated free acid.
Elimination
Elimination of radiolabeled drug is essentially complete within 72 hours, with 90% to 95% of the radioactivity appearing in urine and 5% to 10% in the feces. Clearance of flumazenil occurs primarily by hepatic metabolism and is dependent on hepatic blood flow. In pharmacokinetic studies of normal volunteers, total clearance ranged from 0.8 to 1 L/hr/kg.
Pharmacokinetic parameters following a 5-minute infusion of a total of 1 mg of flumazenil mean (coefficient of variation, range):
C max (ng/mL) | 24 (38%, 11 to 43) |
AUC (ng•hr/mL) | 15 (22%, 10 to 22) |
V ss (L/kg) | 1 (24%, 0.8 to 1.6) |
Cl (L/hr/kg) | 1 (20%, 0.7 to 1.4) |
Half-life (min) | 54 (21%, 41 to 79) |
Food Effects
Ingestion of food during an intravenous infusion of the drug results in a 50% increase in clearance, most likely due to the increased hepatic blood flow that accompanies a meal.
Special Populations
The Elderly
The pharmacokinetics of flumazenil are not significantly altered in the elderly.
Gender
The pharmacokinetics of flumazenil are not different in male and female subjects.
Renal Failure (creatinine clearance <10 mL/min) and Hemodialysis
The pharmacokinetics of flumazenil are not significantly affected.
Patients With Liver Dysfunction
For patients with moderate liver dysfunction, their mean total clearance is decreased to 40% to 60% and in patients with severe liver dysfunction, it is decreased to 25% of normal value, compared with age-matched healthy subjects. This results in a prolongation of the half-life to 1.3 hours in patients with moderate hepatic impairment and 2.4 hours in severely impaired patients. Caution should be exercised with initial and/or repeated dosing to patients with liver disease.
Drug-Drug Interaction
The pharmacokinetic profile of flumazenil is unaltered in the presence of benzodiazepine agonists and the kinetic profiles of those benzodiazepines studied (i.e., diazepam, flunitrazepam, lormetazepam, and midazolam) are unaltered by flumazenil. During the 4-hour steady-state and post infusion of ethanol, there were no pharmacokinetic interactions on ethanol mean plasma levels as compared to placebo when flumazenil doses were given intravenously (at 2.5 hours and 6 hours) nor were interactions of ethanol on the flumazenil elimination half-life found.
Pharmacokinetics in Pediatric Patients
The pharmacokinetics of flumazenil have been evaluated in 29 pediatric patients ranging in age from 1 to 17 years who had undergone minor surgical procedures. The average doses administered were 0.53 mg (0.044 mg/kg) in patients aged 1 to 5 years, 0.63 mg (0.020 mg/kg) in patients aged 6 to 12 years, and 0.8 mg (0.014 mg/kg) in patients aged 13 to 17 years. Compared to adults, the half-life was somewhat shorter and more variable in these patients, averaging 40 minutes and generally ranging from 20 to 75 minutes. Clearance and volume of distribution, normalized for body weight, were in the same range as those seen in adults, although more variability was seen in the pediatric patients.
HOW SUPPLIED
Product Code | Unit of Sale | Strength | Each |
402405 | NDC 63323-424-05 Unit of 10 | 0.5 mg per 5 mL (0.1 mg per mL) | NDC 63323-424-01 5 mL Multiple Dose Vial |
402410 | NDC 63323-424-10 Individually packaged | 1 mg per 10 mL (0.1 mg per mL) | NDC 63323-424-10 10 mL Multiple Dose Vial |
The container closure is not made with natural rubber latex.
Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature].