Get your patient on Fluorometholone - Fluorometholone solution/ Drops (Fluorometholone)
Fluorometholone - Fluorometholone solution/ Drops prescribing information
INDICATIONS AND USAGE
Fluorometholone ophthalmic suspension 0.1% is indicated for the treatment of corticosteroid-responsive inflammation of the palpebral and bulbar conjunctiva, cornea and anterior segment of the globe.
DOSAGE AND ADMINISTRATION
Shake well before using. Instill one drop into the conjunctival sac two to four times daily. During the initial 24 to 48 hours, the dosing frequency may be increased to one application every four hours. Care should be taken not to discontinue therapy prematurely.
If signs and symptoms fail to improve after two days, the patient should be re-evaluated (see PRECAUTIONS ).
The dosing of fluorometholone ophthalmic suspension 0.1% may be reduced, but care should be taken not to discontinue therapy prematurely. In chronic conditions, withdrawal of treatment should be carried out by gradually decreasing the frequency of applications.
CONTRAINDICATIONS
Fluorometholone ophthalmic suspension 0.1% is contraindicated in most viral diseases of the cornea and conjunctiva, including epithelial herpes simplex keratitis (dendritic keratitis), vaccinia, and varicella, and also in mycobacterial infection of the eye, and fungal diseases of ocular structures. Fluorometholone ophthalmic suspension 0.1% is also contraindicated in individuals with known or suspected hypersensitivity to any of the ingredients of this preparation and to other corticosteroids.
ADVERSE REACTIONS
Adverse reactions include, in decreasing order of frequency, elevation of intraocular pressure (IOP) with possible development of glaucoma and infrequent optic nerve damage, posterior subcapsular cataract formation, and delayed wound healing.
Although systemic effects are extremely uncommon, there have been rare occurrences of systemic hypercorticoidism after use of topical dermatologic steroids applied to the skin.
Corticosteroid-containing preparations have also been reported to cause acute anterior uveitis and perforation of the globe. Keratitis, conjunctivitis, corneal ulcers, mydriasis, conjunctival hyperemia, loss of accommodation and ptosis have occasionally been reported following local use of corticosteroids.
The development of secondary ocular infection (bacterial, fungal and viral) has occurred. Fungal and viral infections of the cornea are particularly prone to develop coincidentally with long-term applications of steroids. The possibility of fungal invasion should be considered in any persistent corneal ulceration where steroid treatment has been used (see WARNINGS ).
Transient burning and stinging upon instillation and other minor symptoms of ocular irritation have been reported with the use of fluorometholone suspension.
Other adverse events reported with the use of fluorometholone include: allergic reactions; foreign body sensation; erythema of eyelid; eyelid edema/eye swelling; eye discharge; eye pain; eye pruritus; lacrimation increased; rash; taste perversion; visual disturbance (blurry vision); and visual field defect.
DESCRIPTION
Fluorometholone ophthalmic suspension, USP 0.1% is a sterile topical anti-inflammatory agent for ophthalmic use.
Chemical Name
Fluorometholone: 9-Fluoro-11β,17-dihydroxy-6α-methylpregna-1,4-diene-3,20-dione.
Contains
Active: fluorometholone 0.1%. Preservative: benzalkonium chloride 0.004%. Inactives: edetate disodium; polysorbate 80; polyvinyl alcohol 1.4%; purified water; sodium chloride; sodium phosphate, dibasic; sodium phosphate, monobasic; and sodium hydroxide to adjust pH. Fluorometholone suspension is formulated with a pH from 6.2 to 7.5. It has an osmolality range of 290-350 mOsm/kg.
Structural Formula
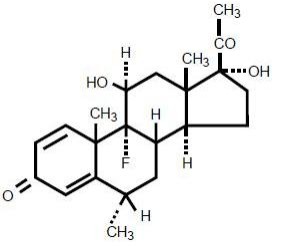
f luorometholone
CLINICAL PHARMACOLOGY
Corticosteroids inhibit the inflammatory response to a variety of inciting agents and probably delay or slow healing. They inhibit the edema, fibrin deposition, capillary dilation, leukocyte migration, capillary proliferation, fibroblast proliferation, deposition of collagen, and scar formation associated with inflammation.
There is no generally accepted explanation for the mechanism of action of ocular corticosteroids. However, corticosteroids are thought to act by the induction of phospholipase A 2 inhibitory proteins, collectively called lipocortins. It is postulated that these proteins control the biosynthesis of potent mediators of inflammation such as prostaglandins and leukotrienes by inhibiting the release of their common precursor, arachidonic acid. Arachidonic acid is released from membrane phospholipids by phospholipase A 2 .
Corticosteroids are capable of producing a rise in intraocular pressure. In clinical studies of documented steroid-responders, fluorometholone demonstrated a significantly longer average time to produce a rise in intraocular pressure than dexamethasone phosphate; however, in a small percentage of individuals, a significant rise in intraocular pressure occurred within one week. The ultimate magnitude of the rise was equivalent for both drugs.
HOW SUPPLIED
Fluorometholone ophthalmic suspension, USP 0.1% is supplied sterile in opaque white LDPE plastic bottles with white high impact polystyrene (HIPS) caps as follows:
5 mL in 10 mL bottle NDC 60758-880-05
10 mL in 15 mL bottle NDC 60758-880-10
15 mL in 15 mL bottle NDC 60758-880-15
Storage:
Store at 2°-25°C (36°-77°F); protect from freezing. Store in an upright position.
Revised : 12/2018
For more information, call 1-800-678-1605
Distributed for: Allergan USA, Inc. Madison, NJ 07940
© 2018 Allergan. All rights reserved.
All trademarks are the property of their respective owners.
v1.0USPI880