Ibuprofen - Ibuprofen suspension prescribing information
Cardiovascular Thrombotic Events
- Nonsteroidal anti-inflammatory drugs (NSAIDs) cause an increased risk of serious cardiovascular thrombotic events, including myocardial infarction and stroke, which can be fatal. This risk may occur early in treatment and may increase with duration of use (see WARNINGS and PRECAUTIONS ).
- Ibuprofen oral suspension is contraindicated in the setting of coronary artery bypass graft (CABG) surgery (see CONTRAINDICATIONS and WARNINGS ).
Gastrointestinal Risk
- NSAIDs cause an increased risk of serious gastrointestinal adverse events including bleeding, ulceration, and perforation of the stomach or intestines, which can be fatal. These events can occur at any time during use and without warning symptoms. Elderly patients are at greater risk for serious gastrointestinal events (see WARNINGS ).
INDICATIONS AND USAGE
Carefully consider the potential benefits and risks of ibuprofen oral suspension and other treatment options before deciding to use ibuprofen. Use the lowest effective dose for the shortest duration consistent with individual patient treatment goals (see WARNINGS ).
In Pediatric Patients, Ibuprofen Oral Suspension is indicated:
- For reduction of fever in patients aged 6 months up to 2 years of age.
- For relief of mild to moderate pain in patients aged 6 months up to 2 years of age.
- For relief of signs and symptoms of juvenile arthritis.
In Adults, Ibuprofen Oral Suspension is indicated:
- For treatment of primary dysmenorrhea.
- For relief of the signs and symptoms of rheumatoid arthritis and osteoarthritis.
Since there have been no controlled trials to demonstrate whether there is any beneficial effect or harmful interaction with the use of ibuprofen in conjunction with aspirin, the combination cannot be recommended (see PRECAUTIONS-Drug Interactions ).
DOSAGE AND ADMINISTRATION
Carefully consider the potential benefits and risks of ibuprofen oral suspension and other treatment options before deciding to use ibuprofen oral suspension. Use the lowest effective dose for the shortest duration consistent with individual patient treatment goals (see WARNINGS ).
After observing the response to initial therapy with ibuprofen oral suspension, the dose and frequency should be adjusted to suit an individual patient's needs.
Pediatric Patients
Fever Reduction
For reduction of fever in children, 6 months up to 2 years of age, the dosage should be adjusted on the basis of the initial temperature level (see CLINICAL PHARMACOLOGY ). The recommended dose is 5 mg/kg if the baseline temperature is less than 102.5ºF, or 10 mg/kg if the baseline temperature is 102.5ºF or greater. The duration of fever reduction is generally 6 to 8 hours. The recommended maximum daily dose is 40 mg/kg.
Analgesia
For relief of mild to moderate pain in children 6 months up to 2 years of age, the recommended dosage is 10 mg/kg, every 6 to 8 hours. The recommended maximum daily dose is 40 mg/kg. Doses should be given so as not to disturb the child's sleep pattern.
Juvenile Arthritis
The recommended dose is 30 to 40 mg/kg/day divided into three to four doses (see Individualization of Dosage ). Patients with milder disease may be adequately treated with 20 mg/kg/day. In patients with juvenile arthritis, doses above 50 mg/kg/day are not recommended because they have not been studied and doses exceeding the upper recommended dose of 40 mg/kg/day may increase the risk of causing serious adverse events. The therapeutic response may require from a few days to several weeks to be achieved. Once a clinical effect is obtained, the dosage should be lowered to the smallest dose of ibuprofen oral suspension needed to maintain adequate control of symptoms.
Pediatric patients receiving doses above 30 mg/kg/day or if abnormal liver function tests have occurred with previous NSAID treatments should be carefully followed for signs and symptoms of early liver dysfunction.
Adults
Primary Dysmenorrhea
For the treatment of primary dysmenorrhea, beginning with the earliest onset of such pain, ibuprofen oral suspension should be given in a dose of 400 mg every 4 hours, as necessary, for the relief of pain.
Rheumatoid Arthritis and Osteoarthritis
Suggested dosage: 1200 to 3200 mg daily (300 mg q.i.d. or 400 mg, 600 mg or 800 mg t.i.d. or q.i.d.). Individual patients may show a better response to 3200 mg daily, as compared with 2400 mg, although in well-controlled clinical trials patients on 3200 mg did not show a better mean response in terms of efficacy. Therefore, when treating patients with 3200 mg/day, the physician should observe sufficient increased clinical benefits to offset potential increased risk.
Individualization of Dosage
The dose of ibuprofen oral suspension should be tailored to each patient, and may be lowered or raised from the suggested doses depending on the severity of symptoms either at time of initiating drug therapy or as the patient responds or fails to respond. One fever study showed that, after the initial dose of ibuprofen oral suspension, subsequent doses may be lowered and still provide adequate fever control.
In a situation when low fever would require the ibuprofen oral suspension 5 mg/kg dose in a child with pain, the dose that will effectively treat the predominant symptom should be chosen. In chronic conditions, a therapeutic response to ibuprofen therapy is sometimes seen in a few days to a week, but most often is observed by two weeks. After a satisfactory response has been achieved, the patient's dose should be reviewed and adjusted as required. Patients with rheumatoid arthritis seem to require higher doses than do patients with osteoarthritis. The smallest dose of ibuprofen oral suspension that yields acceptable control should be employed. Ibuprofen oral suspension may be used in combination with gold salts and/or corticosteroids.
CONTRAINDICATIONS
Ibuprofen oral suspension is contraindicated in patients with known hypersensitivity to ibuprofen.
Ibuprofen should not be given to patients who have experienced asthma, urticaria, or allergic-type reactions after taking aspirin or other NSAIDs. Severe, rarely fatal, anaphylactic-like reactions to NSAIDs have been reported in such patients (see WARNINGS-Anaphylactoid Reactions , and PRECAUTIONS-Preexisting Asthma ).
Ibuprofen is contraindicated in the setting of coronary artery bypass graft (CABG) surgery (see WARNINGS ).
ADVERSE REACTIONS
In patients taking ibuprofen or other NSAIDs, the most frequently reported adverse experiences occurring in approximately 1 to 10% of patients are: Abnormal renal function, anemia, dizziness, edema, elevated liver enzymes, fluid retention, gastrointestinal experiences (including abdominal pain, bloating, constipation, diarrhea, dyspepsia, epigastric pain, flatulence, heartburn, nausea, vomiting), headaches, increased bleeding time, nervousness, pruritus, rashes (including maculopapular) and tinnitus.
Additional adverse experiences reported occasionally include:
Body as a whole - fever, infection, sepsis
Cardiovascular system - congestive heart failure in patients with marginal cardiac function, hypertension, tachycardia, syncope
Digestive system - dry mouth, duodenitis, esophagitis, gastric or duodenal ulcer with bleeding and/or perforation, gastritis, gastrointestinal bleeding, glossitis, hematemesis, hepatitis, jaundice, melena, rectal bleeding
Hemic and lymphatic system - ecchymosis, eosinophilia, leukopenia, purpura, stomatitis, thrombocytopenia
Metabolic and nutritional - weight changes
Nervous system - anxiety, asthenia, confusion, depression, dream abnormalities, drowsiness, insomnia, malaise, paresthesia, somnolence, tremors, vertigo
Respiratory system - asthma, dyspnea
Skin and appendages - alopecia, photosensitivity, sweat
Special senses - blurred vision
Urogenital system - cystitis, dysuria, hematuria, interstitial nephritis, oliguria/polyuria, proteinuria, acute renal failure in patients with pre-existing significantly impaired renal function
Other adverse reactions, which occur rarely are:
Body as a whole - anaphylactic reactions, anaphylactoid reactions, appetite changes
Cardiovascular system - arrhythmia, cerebrovascular accident, hypotension, myocardial infarction, palpitations, vasculitis
Digestive system - eructation, gingival ulcer, hepatorenal syndrome, liver necrosis, liver failure, pancreatitis
Hemic and lymphatic system - agranulocystosis, hemolytic anemia, aplastic anemia, lymphadenopathy, neutropenia, pancytopenia
Metabolic and nutritional - hyperglycemia
Nervous system - convulsions, coma, emotional liability hallucinations, aseptic meningitis
Respiratory - apnea, respiratory depression, pneumonia, rhinitis
Skin and appendages - angioedema, toxic epidermal necrosis, erythema multiforme, exfoliative dermatitis, Stevens Johnson Syndrome, fixed drug eruption (FDE), urticaria, vesiculobullous eruptions
Special senses - amblyopia (blurred and/or diminished vision, scotomata and/or changes in color vision), conjunctivitis, dry eyes, hearing impairment
Urogenital - azotemia, decreased creatinine clearance, glomerulitis, renal papillary necrosis, tubular necrosis
To report SUSPECTED ADVERSE EVENTS, contact Sun Pharmaceutical Industries, Inc., at 1-866-923-4914 or FDA at 1-800-FDA-1088 or http://www.fda.gov/medwatch for voluntary reporting of adverse reactions.
Drug Interactions
ACE-Inhibitors
Reports suggest that NSAIDs may diminish the antihypertensive effect of ACE-inhibitors. This interaction should be given consideration in patients taking NSAIDs concomitantly with ACE-inhibitors.
Aspirin
Pharmacodynamic studies have demonstrated interference with the antiplatelet activity of aspirin when ibuprofen 400 mg, given three times daily, is administered with enteric-coated low-dose aspirin. The interaction exists even following a once-daily regimen of ibuprofen 400 mg, particularly when ibuprofen is dosed prior to aspirin. The interaction is alleviated if immediate-release low-dose aspirin is dosed at least 2 hours prior to a once-daily regimen of ibuprofen; however, this finding cannot be extended to enteric-coated low-dose aspirin (see CLINICAL PHARMACOLOGY-Pharmacodynamics ) .
Because there may be an increased risk of cardiovascular events due to the interference of ibuprofen with the antiplatelet effect of aspirin, for patients taking low-dose aspirin for cardioprotection who require analgesics, consider use of an NSAID that does not interfere with the antiplatelet effect of aspirin, or non-NSAID analgesics, where appropriate.
As with other NSAIDs, concomitant administration of ibuprofen and aspirin is not generally recommended because of the potential of increased adverse effects.
Diuretics
Clinical studies, as well as post marketing observations, have shown that ibuprofen can reduce the natriuretic effect of furosemide and thiazides in some patients. This response has been attributed to inhibition of renal prostaglandin synthesis. During concomitant therapy with NSAIDs, the patient should be observed closely for signs of renal failure (see WARNINGS, Renal Effects ), as well as to assure diuretic efficacy.
Lithium
Ibuprofen produced an elevation of plasma lithium levels and a reduction in renal lithium clearance in a study of eleven normal volunteers. The mean minimum lithium concentration increased 15% and the renal clearance of lithium was decreased by 19% during this period of concomitant drug administration. This effect has been attributed to inhibition of renal prostaglandin synthesis by ibuprofen. Thus, when ibuprofen and lithium are administered concurrently, subjects should be observed carefully for signs of lithium toxicity. (Read circulars for lithium preparation before use of such concurrent therapy.)
Methotrexate
NSAIDs have been reported to competitively inhibit methotrexate accumulation in rabbit kidney slices. This may indicate that they could enhance the toxicity of methotrexate. Caution should be used when NSAIDs are administered concomitantly with methotrexate.
Warfarin
Several short-term controlled studies failed to show that ibuprofen significantly affected prothrombin times or a variety of other clotting factors when administered to individuals on warfarin-type anticoagulants. However, because bleeding has been reported when ibuprofen and other NSAIDs have been administered to patients on warfarin-type anticoagulants, the physician should be cautious when administering ibuprofen to patients on anticoagulants. The effects of warfarin and NSAIDs on GI bleeding are synergistic, such that the users of both drugs together have a risk of serious GI bleeding higher than users of either drug alone.
DESCRIPTION
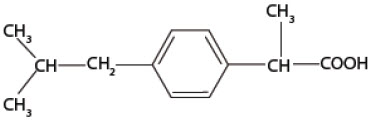
The active ingredient in ibuprofen oral suspension USP is ibuprofen, which is a member of the propionic acid group of nonsteroidal anti-inflammatory drugs (NSAIDs). Ibuprofen is a racemic mixture of [+]S- and [-]R-enantiomers. It is a white to off-white crystalline powder, with a melting point of 74° to 77°C. It is practically insoluble in water (< 0.1 mg/mL), but readily soluble in organic solvents such as ethanol and acetone. Ibuprofen, USP has a pKa of 4.43 ± 0.03 and an n-octanol/water partition coefficient of 11.7 at pH 7.4. The chemical name for ibuprofen is (±)-2-( p -Isobutylphenyl) propionic acid. The molecular weight of ibuprofen is 206.28. Its molecular formula is C 13 H 18 O 2 and it has the following structural formula:
Ibuprofen oral suspension USP is a sucrose-sweetened, white to off-white, berry-flavored suspension containing 100 mg of ibuprofen in 5 mL (20 mg/mL). Inactive ingredients include: acesulfame potassium, berry flavor natural & artificial, citric acid anhydrous, glycerin, pregelatinized modified starch, polysorbate 80, sodium benzoate, purified water, sucrose, xanthan gum.
Meets USP Dissolution Test 2.
CLINICAL PHARMACOLOGY
Pharmacodynamics
Ibuprofen is a nonsteroidal anti-inflammatory drug (NSAID) that possesses anti-inflammatory, analgesic and antipyretic activity. Its mode of action, like that of other NSAIDs, is not completely understood, but may be related to prostaglandin synthetase inhibition. After absorption of the racemic ibuprofen, the [-]R-enantiomer undergoes interconversion to the [+]S-form. The biological activities of ibuprofen are associated with the [+]S-enantiomer.
In a healthy volunteer study, ibuprofen 400 mg given once daily, administered 2 hours prior to immediate-release aspirin (81 mg) for 6 days, showed an interaction with the antiplatelet activity of aspirin as measured by % serum thromboxane B2 (TxB2) inhibition at 24 hours following the day-6 aspirin dose [53%]. An interaction was still observed, but minimized, when ibuprofen 400 mg given once-daily was administered as early as 8 hours prior to the immediate-release aspirin dose [90.7%]. However, there was no interaction with the antiplatelet activity of aspirin when ibuprofen 400 mg, given once daily, was administered 2 hours after (but not concomitantly, 15 min, or 30 min after) the immediate-release aspirin dose [99.2%].
In another study, where immediate-release aspirin 81 mg was administered once daily with ibuprofen 400 mg given three times daily (1, 7, and 13 hours post-aspirin dose) for 10 consecutive days, the mean % serum thromboxane B2 (TxB2) inhibition suggested no interaction with the antiplatelet activity of aspirin [98.3%]. However, there were individual subjects with serum TxB2 inhibition below 95%, with the lowest being 90.2%.
When a similarly designed study was conducted with enteric-coated aspirin, where healthy subjects were administered enteric-coated aspirin 81 mg once daily for 6 days and ibuprofen 400 mg three times daily (2, 7 and 12 h post-aspirin dose) for 6 days, there was an interaction with the antiplatelet activity at 24 hours following the day-6 aspirin dose [67%] (see PRECAUTIONS-Drug Interactions ).
Pharmacokinetics
Ibuprofen is a racemic mixture of [-]R-and [+]S-isomers.
In vivo and in vitro studies indicate that the [+]S-isomer is responsible for clinical activity. The [-]R-form, while thought to be pharmacologically inactive, is slowly and incompletely (~ 60%) interconverted into the active [+]S species in adults. The degree of interconversion in children is unknown, but is thought to be similar. The [-]R-isomer serves as a circulating reservoir to maintain levels of active drug. Ibuprofen is well absorbed orally, with less than 1% being excreted in the urine unchanged. It has a biphasic elimination time curve with a plasma half-life of approximately 2 hours.
Studies in febrile children have established the dose-proportionality of 5 and 10 mg/kg doses of ibuprofen. Studies in adults have established the dose-proportionality of ibuprofen as a single oral dose from 50 to 600 mg for total drug and up to 1200 mg for free drug.
Absorption
In vivo studies indicate that ibuprofen is well absorbed orally from the suspension formulation, with peak plasma levels usually occurring within 1 to 2 hours (see Table 1 ).
| Dose | 200 mg (2.8 mg/kg) in Adults | 10 mg/kg in Febrile Children |
|---|---|---|
| Formulation | Suspension | Suspension |
| Legend: AUC inf = Area-under-the-curve to infinity T max = Time-to-peak plasma concentration C max = Peak plasma concentration Cl/F = Clearance divided by fraction at drug absorbed | ||
| Number of Patients | 24 | 18 |
| AUC inf (mcg∙h/mL) | 64 (27%) | 155 (24%) |
| C max (mcg/mL) | 19 (22%) | 55 (23%) |
| T max (h) | 0.79 (69%) | 0.97 (57%) |
| Cl/F (mg/h/kg) | 45.6 (22%) | 68.6 (22%) |
Antacids
A bioavailability study in adults has shown that there was no interference with the absorption of ibuprofen when given in conjunction with an antacid containing both aluminum hydroxide and magnesium hydroxide.
H-2 Antagonists
In studies with human volunteers, coadministration of cimetidine or ranitidine with ibuprofen had no substantive effect on ibuprofen serum concentrations.
Food Effects
Absorption is most rapid when ibuprofen is given under fasting conditions.
Administration of ibuprofen with food affects the rate but not the extent of absorption. When taken with food, T max is delayed by approximately 30 to 60 minutes, and peak levels are reduced by approximately 30 to 50%.
Distribution
Ibuprofen, like most drugs of its class, is highly protein bound (>99% bound at 20 mcg/mL). Protein binding is saturable and at concentrations >20 mcg/mL binding is non-linear. Based on oral dosing data there is an age- or fever-related change in volume of distribution for ibuprofen. Febrile children <11 years old have a volume of approximately 0.2 L/kg while adults have a volume of approximately 0.12 L/kg. The clinical significance of these findings is unknown.
Metabolism
Following oral administration, the majority of the dose was recovered in the urine within 24 hours as the hydroxy-(25%) and carboxypropyl-(37%) phenylpropionic acid metabolites. The percentages of free and conjugated ibuprofen found in the urine were approximately 1% and 14%, respectively. The remainder of the drug was found in the stool as both metabolites and unabsorbed drug.
Elimination
Ibuprofen is rapidly metabolized and eliminated in the urine. The excretion of ibuprofen is virtually complete 24 hours after the last dose. It has a biphasic plasma elimination time curve with a half-life of approximately 2 hours. There is no difference in the observed terminal elimination rate or half-life between children and adults, however, there is an age- or fever-related change in total clearance. This suggests that the observed change in clearance is due to changes in the volume of distribution of ibuprofen (see Table 1 for Cl/F values).
Clinical Studies
Controlled clinical trials comparing doses of 5 and 10 mg/kg ibuprofen suspension and 10 to 15 mg/kg of acetaminophen elixir have been conducted in children 6 months to 12 years of age with fever primarily due to viral illnesses. In these studies there were no differences between treatments in fever reduction for the first hour and maximum fever reduction occurred between 2 and 4 hours. Response after 1 hour was dependent on both the level of temperature elevation as well as the treatment. In children with baseline temperatures at or below 102.5°F both ibuprofen doses and acetaminophen were equally effective in their maximum effect. In children with temperatures above 102.5°F, the ibuprofen 10 mg/kg dose was more effective. By 6 hours, children treated with ibuprofen 5 mg/kg tended to have recurrence of fever, whereas children treated with ibuprofen 10 mg/kg still had significant fever reduction at 8 hours. In control groups treated with 10 mg/kg acetaminophen, fever reduction resembled that seen in children treated with 5 mg/kg of ibuprofen, with the exception that temperature elevation tended to return 1 to 2 hours earlier.
In patients with primary dysmenorrhea, ibuprofen has been shown to reduce elevated levels of prostaglandin activity in the menstrual fluid and to reduce testing and active intrauterine pressure, as well as the frequency of uterine contractions. The probable mechanism of action is to inhibit prostaglandin synthesis rather than simply to provide analgesia.
Clinical Studies
Controlled clinical trials comparing doses of 5 and 10 mg/kg ibuprofen suspension and 10 to 15 mg/kg of acetaminophen elixir have been conducted in children 6 months to 12 years of age with fever primarily due to viral illnesses. In these studies there were no differences between treatments in fever reduction for the first hour and maximum fever reduction occurred between 2 and 4 hours. Response after 1 hour was dependent on both the level of temperature elevation as well as the treatment. In children with baseline temperatures at or below 102.5°F both ibuprofen doses and acetaminophen were equally effective in their maximum effect. In children with temperatures above 102.5°F, the ibuprofen 10 mg/kg dose was more effective. By 6 hours, children treated with ibuprofen 5 mg/kg tended to have recurrence of fever, whereas children treated with ibuprofen 10 mg/kg still had significant fever reduction at 8 hours. In control groups treated with 10 mg/kg acetaminophen, fever reduction resembled that seen in children treated with 5 mg/kg of ibuprofen, with the exception that temperature elevation tended to return 1 to 2 hours earlier.
In patients with primary dysmenorrhea, ibuprofen has been shown to reduce elevated levels of prostaglandin activity in the menstrual fluid and to reduce testing and active intrauterine pressure, as well as the frequency of uterine contractions. The probable mechanism of action is to inhibit prostaglandin synthesis rather than simply to provide analgesia.
HOW SUPPLIED
Ibuprofen Oral Suspension USP, 100 mg/5 mL
White to off-white, berry-flavored suspension
- Bottles of 4 fl oz (118 mL) - NDC 51672-1385-8
- Bottles of ONE PINT (473 mL) - NDC 51672-1385-9
Shake well before using. Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature].
Dispense in a well-closed container as defined in the USP.