Get your patient on Ipratropium Bromide And Albuterol Sulfate - Ipratropium Bromide And Albuterol Sulfate solution (Ipratropium Bromide And Albuterol Sulfate)
Ipratropium Bromide And Albuterol Sulfate - Ipratropium Bromide And Albuterol Sulfate solution prescribing information
INDICATIONS AND USAGE
Ipratropium Bromide and Albuterol Sulfate Inhalation Solution is indicated for the treatment of bronchospasm associated with COPD in patients requiring more than one bronchodilator.
DOSAGE AND ADMINISTRATION
The recommended dose of Ipratropium Bromide and Albuterol Sulfate Inhalation Solution is one 3 mL vial administered 4 times per day via nebulization with up to 2 additional 3 mL doses allowed per day, if needed. Safety and efficacy of additional doses or increased frequency of administration of Ipratropium Bromide and Albuterol Sulfate Inhalation Solution beyond these guidelines has not been studied and the safety and efficacy of extra doses of albuterol sulfate or ipratropium bromide in addition to the recommended doses of Ipratropium Bromide and Albuterol Sulfate Inhalation Solution have not been studied.
The use of Ipratropium Bromide and Albuterol Sulfate Inhalation Solution can be continued as medically indicated to control recurring bouts of bronchospasm. If a previously effective regimen fails to provide the usual relief, medical advice should be sought immediately, as this is often a sign of worsening COPD, which would require reassessment of therapy.
A Pari-LC-Plus™ nebulizer (with face mask or mouthpiece) connected to a PRONEB™ compressor was used to deliver Ipratropium Bromide and Albuterol Sulfate Inhalation Solution to each patient in one U.S. clinical study. The safety and efficacy of Ipratropium Bromide and Albuterol Sulfate Inhalation Solution delivered by other nebulizers and compressors have not been established.
Ipratropium Bromide and Albuterol Sulfate Inhalation Solution should be administered via jet nebulizer connected to an air compressor with an adequate air flow, equipped with a mouthpiece or suitable face mask.
CONTRAINDICATIONS
Ipratropium Bromide and Albuterol Sulfate Inhalation Solution is contraindicated in patients with a history of hypersensitivity to any of its components, or to atropine and its derivatives.
ADVERSE REACTIONS
Adverse reaction information concerning Ipratropium Bromide and Albuterol Sulfate Inhalation Solution was derived from the 12-week controlled clinical trial.
| Body System COSTART Term | Albuterol n (%) | Ipratropium n (%) | Ipratropium and Albuterol n (%) |
|---|---|---|---|
| NUMBER OF PATIENTS | 761 | 754 | 765 |
| N (%) Patients with AE | 327 (43.0) | 329 (43.6) | 367 (48.0) |
| BODY AS A WHOLE | |||
| Pain | 8 (1.1) | 4 (0.5) | 10 (1.3) |
| Pain chest | 11 (1.4) | 14 (1.9) | 20 (2.6) |
| DIGESTIVE | |||
| Diarrhea | 5 (0.7) | 9 (1.2) | 14 (1.8) |
| Dyspepsia | 7 (0.9) | 8 (1.1) | 10 (1.3) |
| Nausea | 7 (0.9) | 6 (0.8) | 11 (1.4) |
| MUSCULO-SKELETAL | |||
| Cramps leg | 8 (1.1) | 6 (0.8) | 11 (1.4) |
| RESPIRATORY | |||
| Bronchitis | 11 (1.4) | 13 (1.7) | 13 (1.7) |
| Lung Disease | 36 (4.7) | 34 (4.5) | 49 (6.4) |
| Pharyngitis | 27 (3.5) | 27 (3.6) | 34 (4.4) |
| Pneumonia | 7 (0.9) | 8 (1.1) | 10 (1.3) |
| UROGENITAL | |||
| Infection urinary tract | 3 (0.4) | 9 (1.2) | 12 (1.6) |
Additional adverse reactions reported in more than 1% of patients treated with Ipratropium Bromide and Albuterol Sulfate Inhalation Solution included constipation and voice alterations.
In the clinical trial, there was a 0.3% incidence of possible allergic-type reactions, including skin rash, pruritus, and urticaria.
Additional information derived from the published literature on the use of albuterol sulfate and ipratropium bromide singly or in combination includes precipitation or worsening of narrow-angle glaucoma, acute eye pain, blurred vision, mydriasis, paradoxical bronchospasm, wheezing, exacerbation of COPD symptoms, drowsiness, aching, flushing, upper respiratory tract infection, palpitations, taste perversion, elevated heart rate, sinusitis, back pain, sore throat and metabolic acidosis. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Drug Interactions
Anticholinergic agents
Although ipratropium bromide is minimally absorbed into the systemic circulation, there is some potential for an additive interaction with concomitantly used anticholinergic medications. Caution is, therefore, advised in the co-administration of Ipratropium Bromide and Albuterol Sulfate Inhalation Solution with other drugs having anticholinergic properties.
β-adrenergic agents
Caution is advised in the co-administration of Ipratropium Bromide and Albuterol Sulfate Inhalation Solution and other sympathomimetic agents due to the increased risk of adverse cardiovascular effects.
β-receptor blocking agents
These agents and albuterol sulfate inhibit the effect of each other. β-receptor blocking agents should be used with caution in patients with hyperreactive airways, and if used, relatively selective β 1 selective agents are recommended.
Diuretics
The electrocardiogram (ECG) changes and/or hypokalemia that may result from the administration of non-potassium sparing diuretics (such as loop or thiazide diuretics) can be acutely worsened by β-agonists, especially when the recommended dose of the β-agonist is exceeded. Although the clinical significance of these effects is not known, caution is advised in the co-administration of β-agonist-containing drugs, such as Ipratropium Bromide and Albuterol Sulfate Inhalation Solution, with non-potassium sparing diuretics.
Monoamine oxidase inhibitors or tricyclic antidepressants
Ipratropium Bromide and Albuterol Sulfate Inhalation Solution should be administered with extreme caution to patients being treated with monoamine oxidase inhibitors or tricyclic antidepressants, or within 2 weeks of discontinuation of such agents because the action of albuterol sulfate on the cardiovascular system may be potentiated.
DESCRIPTION
The active components in Ipratropium Bromide and Albuterol Sulfate Inhalation Solution are albuterol sulfate and ipratropium bromide.
Albuterol sulfate, is a salt of racemic albuterol and a relatively selective β 2 -adrenergic bronchodilator chemically described as α 1 -[( tert -butylamino)methyl]-4-hydroxy- m -xylene-α, α'-diol sulfate (2:1) (salt). It has a molecular weight of 576.7 and the empirical formula is (C 13 H 21 NO 3 ) 2 •H 2 SO 4 . It is a white crystalline powder, soluble in water and slightly soluble in ethanol. The World Health Organization recommended name for albuterol base is salbutamol.
Figure 3.1-1. Chemical structure of albuterol sulfate.
Ipratropium bromide is an anticholinergic bronchodilator chemically described as 8-azoniabicyclo [3.2.1]-octane, 3-(3-hydroxy-1-oxo-2-phenylpropoxy)-8methyl-8-(1-methylethyl)-, bromide, monohydrate ( endo, syn )-, (±)-; a synthetic quaternary ammonium compound, chemically related to atropine. It has a molecular weight of 430.4 and the empirical formula is C 20 H 30 BrNO 3 •H 2 O. It is a white crystalline substance, freely soluble in water and lower alcohols, and insoluble in lipophilic solvents such as ether, chloroform, and fluorocarbons.
Figure 3.1-2. Chemical structure of ipratropium bromide.
Each 3 mL Sterile Unit-dose Vial contains 0.5 mg of ipratropium bromide (0.017%) and 3 mg Equivalent to 2.5 mg albuterol base albuterol sulfate (0.083%) in an isotonic, sterile, aqueous solution containing sodium chloride and 1 N hydrochloric acid to adjust to pH 4.
Ipratropium Bromide and Albuterol Sulfate Inhalation Solution is a clear, colorless solution. It does not require dilution prior to administration by nebulization. For Ipratropium Bromide and Albuterol Sulfate Inhalation Solution, like all other nebulized treatments, the amount delivered to the lungs will depend on patient factors, the jet nebulizer utilized, and compressor performance. Using the Pari-LC-Plus™ nebulizer (with face mask or mouthpiece) connected to a PRONEB™ compressor system, under in vitro conditions, the mean delivered dose from the mouth piece (% nominal dose) was approximately 46% of albuterol and 42% of ipratropium bromide at a mean flow rate of 3.6 L/min. The mean nebulization time was 15 minutes or less. Ipratropium Bromide and Albuterol Sulfate Inhalation Solution should be administered from jet nebulizers at adequate flow rates, via face masks or mouthpieces (see DOSAGE AND ADMINISTRATION ).
CLINICAL PHARMACOLOGY
Ipratropium Bromide and Albuterol Sulfate Inhalation Solution is a combination of the β 2 -adrenergic bronchodilator, albuterol sulfate, and the anticholinergic bronchodilator, ipratropium bromide.
Albuterol sulfate
Mechanism of Action
The prime action of β-adrenergic drugs is to stimulate adenyl cyclase, the enzyme that catalyzes the formation of cyclic-3',5'-adenosine monophosphate (cAMP) from adenosine triphosphate (ATP). The cAMP thus formed mediates the cellular responses. In vitro studies and in vivo pharmacologic studies have demonstrated that albuterol has a preferential effect on β 2 -adrenergic receptors compared with isoproterenol. While it is recognized that β 2 -adrenergic receptors are the predominant receptors in bronchial smooth muscle, recent data indicated that 10% to 50% of the β-receptors in the human heart may be β 2 -receptors. The precise function of these receptors, however, is not yet established. Albuterol has been shown in most controlled clinical trials to have more effect on the respiratory tract, in the form of bronchial smooth muscle relaxation, than isoproterenol at comparable doses while producing fewer cardiovascular effects. Controlled clinical studies and other clinical experience have shown that inhaled albuterol, like other β-adrenergic agonist drugs, can produce a significant cardiovascular effect in some patients.
Pharmacokinetics
Albuterol sulfate is longer acting than isoproterenol in most patients by any route of administration, because it is not a substrate for the cellular uptake processes for catecholamine nor for the metabolism of catechol-O-methyl transferase. Instead the drug is conjugatively metabolized to albuterol 4'- O -sulfate.
Animal Pharmacology/Toxicology
Intravenous studies in rats with albuterol sulfate have demonstrated that albuterol crosses the blood-brain barrier and reaches brain concentrations amounting to approximately 5% of plasma concentrations. In structures outside of the blood-brain barrier (pineal and pituitary glands), albuterol concentrations were found to be 100 times those found in whole brain.
Studies in laboratory animals (minipigs, rodents, and dogs) have demonstrated the occurrence of cardiac arrhythmias and sudden death (with histological evidence of myocardial necrosis) when beta-agonists and methyl-xanthines are administered concurrently. The clinical significance of these findings is unknown.
Ipratropium bromide
Mechanism of Action
Ipratropium bromide is an anticholinergic (parasympatholytic) agent, which blocks the muscarinic receptors of acetylcholine, and, based on animal studies, appears to inhibit vagally mediated reflexes by antagonizing the action of acetylcholine, the transmitter agent released from the vagus nerve. Anticholinergics prevent the increases in intracellular concentration of cyclic guanosine monophosphate (cGMP), resulting from the interaction of acetylcholine with the muscarinic receptors of bronchial smooth muscle.
Pharmacokinetics
The bronchodilation following inhalation of ipratropium is primarily a local, site-specific effect, not a systemic one. Much of an inhaled dose is swallowed as shown by fecal excretion studies. Following nebulization of a 1-mg dose to healthy volunteers, a mean of 4% of the dose was excreted unchanged in the urine.
Ipratropium bromide is minimally (0% to 9% in vitro ) bound to plasma albumin and α 1 -acid glycoproteins. It is partially metabolized to inactive ester hydrolysis products. Following intravenous administration, approximately one-half is excreted unchanged in the urine. The half-life of elimination is about 1.6 hours after intravenous administration. Ipratropium bromide that reaches the systemic circulation is reportedly removed by the kidneys rapidly at a rate that exceeds the glomerular filtration rate. The pharmacokinetics of Ipratropium Bromide and Albuterol Sulfate Inhalation Solution or ipratropium bromide have not been studied in the elderly and in patients with hepatic or renal insufficiency (see PRECAUTIONS ).
Animal Pharmacology/Toxicology
Autoradiographic studies in rats have shown that ipratropium does not penetrate the blood-brain barrier.
Ipratropium Bromide and Albuterol Sulfate Inhalation Solution
Mechanism of Action
Ipratropium Bromide and Albuterol Sulfate Inhalation Solution is expected to maximize the response to treatment in patients with chronic obstructive pulmonary disease (COPD) by reducing bronchospasm through two distinctly different mechanisms: sympathomimetic (albuterol sulfate) and anticholinergic/parasympatholytic (ipratropium bromide). Simultaneous administration of both an anticholinergic and a β2-sympathomimetic is designed to produce greater bronchodilation effects than when either drug is utilized alone at its recommended dosage.
Animal Pharmacology/Toxicology
In 30-day studies in Sprague-Dawley rats and Beagle dogs, subcutaneous doses of up to 205.5 mcg/kg of ipratropium administered with up to 1000 mcg/kg albuterol in rats and 3.16 mcg/kg ipratropium and 15 mcg/kg albuterol in dogs (less than the maximum recommended daily inhalation dose for adults on a mg/m 2 basis) did not cause death or potentiation of the cardiotoxicity induced by albuterol administered alone.
Pharmacokinetics
In a double blind, double period, crossover study, 15 male and female subjects were administered single doses of Ipratropium Bromide and Albuterol Sulfate Inhalation Solution or albuterol sulfate inhalation solution at two times the recommended single doses as two inhalations separated by 15 minutes. The total nebulized dose of albuterol sulfate from both treatments was 6 mg and the total dose of ipratropium bromide from Ipratropium Bromide and Albuterol Sulfate Inhalation Solution was 1 mg. Peak albuterol plasma concentrations occurred at 0.8 hours after dosing for both treatments. The mean peak albuterol concentration following administration of albuterol sulfate alone was 4.86 (± 2.65) mg/mL and it was 4.65 (± 2.92) mg/mL for Ipratropium Bromide and Albuterol Sulfate Inhalation Solution. Mean AUC values for the two treatments were 26.6 (± 15.2) ng∙hr/mL (albuterol sulfate alone) versus 24.2 (± 14.5) ng∙hr/mL (Ipratropium Bromide and Albuterol Sulfate Inhalation Solution). The mean t 1/2 values were 7.2 (± 1.3) hours (albuterol sulfate alone) and 6.7 (± 1.7) hours (Ipratropium Bromide and Albuterol Sulfate Inhalation Solution). A mean of 8.4 (± 8.9)% of the albuterol dose was excreted unchanged in urine following administration of two vials of Ipratropium Bromide and Albuterol Sulfate Inhalation Solution which is similar to 8.8 (± 7.3)% that was obtained from albuterol sulfate inhalation solution. There were no statistically significant differences in the pharmacokinetics of albuterol between the two treatments. For ipratropium, a mean of 3.9 (± 5.1)% of the ipratropium bromide dose was excreted unchanged in urine following two vials of Ipratropium Bromide and Albuterol Sulfate Inhalation Solution, which is comparable with previously reported data.
Clinical Trials
In a 12 week, randomized, double-blind, positive-control, crossover study of albuterol sulfate, ipratropium bromide, and Ipratropium Bromide and Albuterol Sulfate Inhalation Solution, 863 COPD patients were evaluated for bronchodilator efficacy comparing ipratropium bromide and albuterol sulfate with albuterol sulfate and ipratropium bromide alone.
Ipratropium Bromide and Albuterol Sulfate Inhalation Solution demonstrated significantly better changes in FEV 1 , as measured from baseline to peak response, when compared with either albuterol sulfate or ipratropium bromide. Ipratropium Bromide and Albuterol Sulfate Inhalation Solution was also shown to have the rapid onset associated with albuterol sulfate, with a mean time to peak FEV 1 of 1.5 hours, and the extended duration associated with ipratropium bromide with a duration of 15% response in FEV 1 of 4.3 hours.
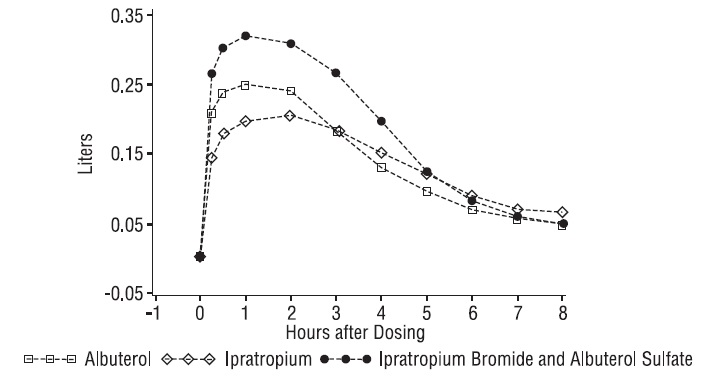
Figure 3. 1-3. Mean Change in FEV 1 - Measured on Day 14
This study demonstrated that each component of Ipratropium Bromide and Albuterol Sulfate Inhalation Solution contributed to the improvement in pulmonary function, especially during the first 4 to 5 hours after dosing, and that Ipratropium Bromide and Albuterol Sulfate Inhalation Solution was significantly more effective than albuterol sulfate or ipratropium bromide alone.
Clinical Trials
In a 12 week, randomized, double-blind, positive-control, crossover study of albuterol sulfate, ipratropium bromide, and Ipratropium Bromide and Albuterol Sulfate Inhalation Solution, 863 COPD patients were evaluated for bronchodilator efficacy comparing ipratropium bromide and albuterol sulfate with albuterol sulfate and ipratropium bromide alone.
Ipratropium Bromide and Albuterol Sulfate Inhalation Solution demonstrated significantly better changes in FEV 1 , as measured from baseline to peak response, when compared with either albuterol sulfate or ipratropium bromide. Ipratropium Bromide and Albuterol Sulfate Inhalation Solution was also shown to have the rapid onset associated with albuterol sulfate, with a mean time to peak FEV 1 of 1.5 hours, and the extended duration associated with ipratropium bromide with a duration of 15% response in FEV 1 of 4.3 hours.
Figure 3. 1-3. Mean Change in FEV 1 - Measured on Day 14
This study demonstrated that each component of Ipratropium Bromide and Albuterol Sulfate Inhalation Solution contributed to the improvement in pulmonary function, especially during the first 4 to 5 hours after dosing, and that Ipratropium Bromide and Albuterol Sulfate Inhalation Solution was significantly more effective than albuterol sulfate or ipratropium bromide alone.
HOW SUPPLIED
Ipratropium Bromide and Albuterol Sulfate Inhalation Solution is supplied as a 3-mL sterile solution for nebulization in sterile low-density polyethylene unit-dose vials. Store in pouch until time of use. Supplied in cartons as listed below.
| NDC 60429-975-30 | 30 vials per carton / 30 vials per foil pouch |
| NDC 60429-975-60 | 60 vials per carton / 30 vials per foil pouch |
Store between 2°C and 25°C (36°F and 77°F). Protect from light.
Mechanism of Action
The prime action of β-adrenergic drugs is to stimulate adenyl cyclase, the enzyme that catalyzes the formation of cyclic-3',5'-adenosine monophosphate (cAMP) from adenosine triphosphate (ATP). The cAMP thus formed mediates the cellular responses. In vitro studies and in vivo pharmacologic studies have demonstrated that albuterol has a preferential effect on β 2 -adrenergic receptors compared with isoproterenol. While it is recognized that β 2 -adrenergic receptors are the predominant receptors in bronchial smooth muscle, recent data indicated that 10% to 50% of the β-receptors in the human heart may be β 2 -receptors. The precise function of these receptors, however, is not yet established. Albuterol has been shown in most controlled clinical trials to have more effect on the respiratory tract, in the form of bronchial smooth muscle relaxation, than isoproterenol at comparable doses while producing fewer cardiovascular effects. Controlled clinical studies and other clinical experience have shown that inhaled albuterol, like other β-adrenergic agonist drugs, can produce a significant cardiovascular effect in some patients.