Isosorbide Dinitrate - Isosorbide Dinitrate tablet prescribing information
INDICATIONS AND USAGE
Isosorbide dinitrate tablets are indicated for the prevention of angina pectoris due to coronary artery disease. The onset of action of immediate-release oral isosorbide dinitrate is not sufficiently rapid for this product to be useful in aborting an acute anginal episode.
DOSAGE AND ADMINISTRATION
As noted under CLINICAL PHARMACOLOGY , multiple-dose studies with ISDN and other nitrates have shown that maintenance of continuous 24-hour plasma levels results in refractory tolerance. Every dosing regimen for isosorbide dinitrate tablets must provide a daily dose-free interval to minimize the development of this tolerance. With immediate-release ISDN, it appears that one daily dose-free interval must be at least 14 hours long.
As also noted under CLINICAL PHARMACOLOGY , the effects of the second and later doses have been smaller and shorter-lasting than the effects of the first.
Large controlled studies with other nitrates suggest that no dosing regimen with isosorbide dinitrate tablets should be expected to provide more than about 12 hours of continuous anti-anginal efficacy per day.
As with all titratable drugs, it is important to administer the minimum dose which produces the desired clinical effect. The usual starting dose of isosorbide dinitrate tablets is 5 mg to 20 mg, two or three times daily. For maintenance therapy, 10 mg to 40 mg, two or three times daily is recommended. Some patients may require higher doses. A daily dose-free interval of at least 14 hours is advisable to minimize tolerance. The optimal interval will vary with the individual patient, dose and regimen.
CONTRAINDICATIONS
Isosorbide dinitrate tablets are contraindicated in patients who are allergic to isosorbide dinitrate or any of its ingredients.
Do not use isosorbide dinitrate in patients who are taking certain drugs for erectile dysfunction (phosphodiesterase inhibitors), such as sildenafil, tadalafil, or vardenafil. Concomitant use can cause severe hypotension, syncope, or myocardial ischemia.
Do not use isosorbide dinitrate in patients who are taking the soluble guanylate cyclase stimulator riociguat. Concomitant use can cause hypotension.
ADVERSE REACTIONS
Adverse reactions to isosorbide dinitrate are generally dose-related, and almost all of these reactions are the result of isosorbide dinitrate's activity as a vasodilator. Headache, which may be severe, is the most commonly reported side effect. Headache may be recurrent with each daily dose, especially at higher doses. Transient episodes of lightheadedness, occasionally related to blood pressure changes, may also occur. Hypotension occurs infrequently, but in some patients it may be severe enough to warrant discontinuation of therapy. Syncope, crescendo angina, and rebound hypertension have been reported but are uncommon.
Extremely rarely, ordinary doses of organic nitrates have caused methemoglobinemia in normal-seeming patients. Methemoglobinemia is so infrequent at these doses that further discussion of its diagnosis and treatment is deferred (see OVERDOSAGE ).
Data are not available to allow estimation of the frequency of adverse reactions during treatment with isosorbide dinitrate tablets.
To report SUSPECTED ADVERSE REACTIONS, contact Zydus Pharmaceuticals (USA)
Inc. at 1-877-993-8779 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
The vasodilating effects of isosorbide dinitrate may be additive with those of other vasodilators. Alcohol, in particular, has been found to exhibit additive effects of this variety.
Concomitant use of isosorbide dinitrate with phosphodiesterase inhibitors in any form is contraindicated (see CONTRAINDICATIONS ).
Concomitant use of isosorbide dinitrate with riociguat, a soluble guanylate cyclase stimulator, is contraindicated (see CONTRAINDICATIONS ).
DESCRIPTION
Isosorbide dinitrate (ISDN) is 1,4:3,6-dianhydro-D-glucitol 2,5-dinitrate, an organic nitrate whose structural formula is
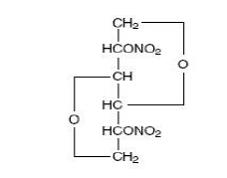
and whose molecular weight is 236.14. The organic nitrates are vasodilators, active on both arteries and veins.
Isosorbide dinitrate is a white, crystalline compound, has a melting point of 70°C and has an optical rotation of +140° (c=1, alcohol, 20°C). Isosorbide dinitrate is very slightly soluble in water; very soluble in acetone and sparingly soluble in alcohol.
Each isosorbide dinitrate tablet, USP contains 5 mg, 10 mg, 20 mg, 30 mg or 40 mg of isosorbide dinitrate. The inactive ingredients in each tablet are lactose monohydrate, magnesium stearate, microcrystalline cellulose, povidone and sodium starch glycolate. The 5 mg dosage strength also contains FD&C red no. 40 aluminium lake. The 20 mg and 40 mg dosage strengths also contain FD&C blue no. 1 aluminium lake and D&C yellow no. 10 aluminium lake. The 30 mg dosage strength also contains FD&C blue no. 1 aluminium lake.
CLINICAL PHARMACOLOGY
The principal pharmacological action of isosorbide dinitrate is relaxation of vascular smooth muscle and consequent dilatation of peripheral arteries and veins, especially the latter. Dilatation of the veins promotes peripheral pooling of blood and decreases venous return to the heart, thereby reducing left ventricular end-diastolic pressure and pulmonary capillary wedge pressure (preload). Arteriolar relaxation reduces systemic vascular resistance, systolic arterial pressure, and mean arterial pressure (afterload). Dilatation of the coronary arteries also occurs. The relative importance of preload reduction, afterload reduction, and coronary dilatation remains undefined.
Dosing regimens for most chronically used drugs are designed to provide plasma concentrations that are continuously greater than a minimally effective concentration. This strategy is inappropriate for organic nitrates. Several well-controlled clinical trials have used exercise testing to assess the anti-anginal efficacy of continuously-delivered nitrates. In the large majority of these trials, active agents were no more effective than placebo after 24 hours (or less) of continuous therapy. Attempts to overcome nitrate tolerance by dose escalation, even to doses far in excess of those used acutely, have consistently failed.
Only after nitrates have been absent from the body for several hours has their anti-anginal efficacy been restored.
Pharmacokinetics
Absorption of isosorbide dinitrate after oral dosing is nearly complete, but bioavailability is highly variable (10% to 90%), with extensive first-pass metabolism in the liver. Serum levels reach their maxima about an hour after ingestion. The average bioavailability of ISDN is about 25%; most studies have observed progressive increases in bioavailability during chronic therapy.
Once absorbed, the volume of distribution of isosorbide dinitrate is 2 L/kg to 4 L/kg, and this volume is cleared at the rate of 2 L/min to 4 L/min, so ISDN's half-life in serum is about an hour. Since the clearance exceeds hepatic blood flow, considerable extra hepatic metabolism must also occur. Clearance is affected primarily by denitration to the 2-mononitrate (15% to 25%) and the 5-mononitrate (75% to 85%).
Both metabolites have biological activity, especially the 5-mononitrate. With an overall half-life of about 5 hours, the 5-mononitrate is cleared from the serum by denitration to isosorbide, glucuronidation to the 5-mononitrate glucuronide, and denitration/hydration to sorbitol. The 2-mononitrate has been less well studied, but it appears to participate in the same metabolic pathways, with a half-life of about 2 hours.
The daily dose-free interval sufficient to avoid tolerance to organic nitrates has not been well defined. Studies of nitroglycerin (an organic nitrate with a very short half-life) have shown that daily dose-free intervals of 10 to 12 hours are usually sufficient to minimize tolerance. Daily dose-free intervals that have succeeded in avoiding tolerance during trials of moderate doses ( e.g. , 30 mg) of immediate-release ISDN have generally been somewhat longer (at least 14 hours), but this is consistent with the longer half-lives of ISDN and its active metabolites.
Few well-controlled clinical trials of organic nitrates have been designed to detect rebound or withdrawal effects. In one such trial, however, subjects receiving nitroglycerin had less exercise tolerance at the end of the daily dose-free interval than the parallel group receiving placebo. The incidence, magnitude, and clinical significance of similar phenomena in patients receiving ISDN have not been studied.
Clinical Trials
In clinical trials, immediate-release oral isosorbide dinitrate has been administered in a variety of regimens, with total daily doses ranging from 30 mg to 480 mg. Controlled trials of single oral doses of isosorbide dinitrate have demonstrated effective reductions in exercise-related angina for up to 8 hours. Anti-anginal activity is present about 1 hour after dosing.
Most controlled trials of multiple-dose oral ISDN taken every 12 hours (or more frequently) for several weeks have shown statistically significant anti-anginal efficacy for only 2 hours after dosing. Once-daily regimens, and regimens with one daily dose-free interval of at least 14 hours ( e.g. , a regimen providing doses at 0800, 1400, and 1800 hours), have shown efficacy after the first dose of each day that was similar to that shown in the single-dose studies cited above. The effects of the second and later doses have been smaller and shorter-lasting than the effect of the first.
From large, well-controlled studies of other nitrates, it is reasonable to believe that the maximal achievable daily duration of anti-anginal effect from isosorbide dinitrate is about 12 hours. No dosing regimen for isosorbide dinitrate, however, has ever actually been shown to achieve this duration of effect. One study of 8 patients, who were administered a pretitrated dose (average 27.5 mg) of immediate-release ISDN at 0800, 1300, and 1800 hours for 2 weeks, revealed that significant anti-anginal effectiveness was discontinuous and totaled about 6 hours in a 24 hour period.
HOW SUPPLIED
Isosorbide dinitrate tablets, USP are available as follows:
Isosorbide dinitrate tablets USP, 5 mg, light pink to pink colored, spotted, round shaped, biconvex, uncoated tablets debossed with "1148" on one side and score on other side.
NDC 70710-1148-1 in bottles of 100 tablets with child-resistant closure
NDC 70710-1148-0 in bottles of 1000 tablets
Isosorbide dinitrate tablets USP, 10 mg, white to off white colored, round shaped, biconvex, uncoated tablets debossed with "1149" on one side and score on other side.
NDC 70710-1149-1 in bottles of 100 tablets with child-resistant closure
NDC 70710-1149-0 in bottles of 1000 tablets
Isosorbide dinitrate tablets USP, 20 mg, light green to green colored, spotted, round shaped, biconvex, uncoated tablets debossed with "1150" on one side and score on other side.
NDC 70710-1150-1 in bottles of 100 tablets with child-resistant closure
NDC 70710-1150-0 in bottles of 1000 tablets
Isosorbide dinitrate tablets USP, 30 mg, light blue to blue colored, spotted, round shaped, biconvex, uncoated tablets debossed with "1151" on one side and score on other side.
NDC 70710-1151-1 in bottles of 100 tablets with child-resistant closure
NDC 70710-1151-0 in bottles of 1000 tablets
Isosorbide dinitrate tablets USP, 40 mg, light green to green colored, spotted, round, biconvex, uncoated tablets, debossed with "1152" on one side and score on other side.
NDC 70710-1152-1 in bottles of 100 tablets with child-resistant closure
Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature].
Protect from Light. Dispense in a light-resistant, tight container.
Keep bottles tightly closed.
Manufactured by:
Zydus Lifesciences Ltd.,
Baddi, India
Distributed by:
Zydus Pharmaceuticals (USA) Inc.
Pennington, NJ 08534
Rev. 12/22