Get your patient on Macrilen (Macimorelin Acetate)
Macrilen prescribing information
INDICATIONS AND USAGE
MACRILEN is indicated for the diagnosis of adult growth hormone deficiency (AGHD).
Limitations of Use
The safety and diagnostic performance of MACRILEN have not been established for subjects with a body mass index (BMI) > 40 kg/m 2 .
DOSAGE AND ADMINISTRATION
- Recommended dose is 0.5 mg/kg as a single oral dose, after fasting for at least 8 hours (2.1 ).
- See Full Prescribing Information for important preparation and administration instructions (2.3 ).
- Discontinue therapy with strong CYP3A4 inducers, growth hormones and drugs that affect GH release for an adequate length of time before administering MACRILEN (2.2 ).
- Adequately replace other hormone deficiencies before administering MACRILEN (2.2 ).
Recommended Dose
The recommended dose is a single oral dose of 0.5 mg/kg of macimorelin. The dose is administered as a reconstituted solution [see Dosage and Administration (2.3 )] in patients fasted for at least 8 hours.
Important Recommendations Before MACRILEN Use
- Discontinue strong CYP3A4 inducers prior to MACRILEN use [see Warning and Precautions (5.2 ) and Drug Interactions (7.2 )].
- Discontinue growth hormone (GH) therapy at least one week before administering MACRILEN [see Drug Interactions (7.3 )] .
- Avoid the use of MACRILEN with drugs known to affect pituitary GH secretion [see Drug Interactions (7.3 )] .
- For patients with deficiencies in sex hormones, thyroid hormone and/or glucocorticoid, adequately replace each of the missing hormones before administering MACRILEN.
- Ensure that the patient has fasted for at least 8 hours before MACRILEN use.
Directions for Preparation and Administration
Prepare and administer by a healthcare professional exactly as follows.
Prepare the MACRILEN solution:
- Weigh the patient in kilograms (i.e., kg) .
- Determine the number of MACRILEN pouches needed to prepare the dose:
- i. For a patient weighing up to 120 kg, use 1 pouch.
- ii. For a patient weighing more than 120 kg, use 2 pouches.
- Use a glass or transparent plastic container with graduation in milliliters (i.e., mL) to dissolve the entire contents of the pouch(es) in the appropriate volume of water.
- i. For 1 pouch dissolve in 120 mL of water (corresponds to 60 mg/120 mL).
- ii. For 2 pouches dissolve in 240 mL of water (corresponds to 120 mg/240 mL).
- Stir the MACRILEN solution gently for about 2 to 3 minutes (a small amount of un-dissolved particles will remain). The solution will have a final concentration of 0.5 mg/mL .
- Use the MACRILEN solution within 30 minutes after preparation.
- Discard any unused MACRILEN solution.
Determine the volume of MACRILEN solution needed for the test:
- Determine the recommended dose to be administered by multiplying the patient weight in kilogram by 0.5 mg/kg.
For example, a 70 kg patient will need a 35 mg dose.
- Determine the volume of prepared MACRILEN solution to be administered by dividing the recommended dose by 0.5 mg/mL.
For example, a patient requiring a dose of 35 mg will need 70 mL of reconstituted MACRILEN solution.
- Use a syringe (without a needle) with graduations in mL to measure the exact volume of MACRILEN solution to be administered and transfer the required volume of MACRILEN solution into a drinking glass.
Administer the MACRILEN solution and perform the test:
- Have the patient being tested drink the entire volume of MACRILEN solution in the drinking glass (i.e., the dose) within 30 seconds .
- Observe the patient being tested per routine for the duration of the test.
- Draw venous blood samples for GH determination at 30 minutes, 45 minutes, 60 minutes and 90 minutes after administration of MACRILEN.
- Prepare serum samples and send to a laboratory for growth hormone determinations.
Interpretation of MACRILEN Test Results
Clinical studies have established that a maximally stimulated serum GH level of less than 2.8 ng/mL (i.e., at the 30, 45, 60 and 90 minute timepoints) following MACRILEN administration confirms the presence of adult growth hormone deficiency.
DOSAGE FORMS AND STRENGTHS
For oral solution: 60 mg white to off-white granules in a pouch for reconstitution in 120 mL of water, resulting in a solution of 0.5 mg/mL of macimorelin.
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk summary
There are no available data with MACRILEN use in pregnant women to inform a drug associated risk for adverse developmental outcomes. Animal reproduction studies have not been conducted with MACRILEN. MACRILEN is indicated as a single dose which limits the risk of adverse developmental outcomes from exposure to MACRILEN.
The estimated background risk of major birth defects and miscarriage for the indicated populations is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 – 4% and 15 – 20%, respectively.
Lactation
Risk Summary
There are no data on the presence of macimorelin in human or animal milk, the effects on the breastfed infant or the effects on milk production. The lack of clinical data during lactation precludes a clear determination of the risk of MACRILEN to an infant during lactation; therefore, the developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for MACRILEN and any potential adverse effects on the breastfed infant from MACRILEN or the underlying maternal condition.
Pediatric Use
The safety and efficacy of MACRILEN in pediatric patients have not been established.
The use of MACRILEN for the diagnosis of Growth Hormone Deficiency (GHD) was evaluated in two open-label studies in pediatric patients aged 3 to 17 years of age.
Study 1 (Phase 2) was an open-label, group comparison, dose-escalation single dose escalation study in 24 pediatric patients with suspected GHD. No serious adverse events (SAEs) and no adverse events (AEs) were associated with the macimorelin growth hormone stimulation test (GHST). The study demonstrated a dose-dependent increase in macimorelin exposure and growth hormone (GH) stimulation.
Study 2 (Phase 3) was a multicenter, open-label, randomized, crossover study in 102 pediatric patients with suspected GHD. Patients received a single oral dose of MACRILEN on two different occasions, compared to two standard growth hormone stimulation tests (arginine and clonidine). The primary efficacy endpoint was the area under the receiver operating characteristic (ROC) curve (AUC) assessing the diagnostic accuracy of MACRILEN compared to the adjudicated GHD status. The study failed to meet its primary endpoint; the lower bound of the 97.5% confidence interval for the ROC AUC was 0.66, which did not meet the pre-specified threshold of >0.70.
Diagnostic performance (sensitivity and specificity) was evaluated against a cut-off point of 25.59 ng/mL, which was derived from the study data. Using this cut-off, sensitivity was 78.6% (95% CI: 63.2, 89.7) and specificity was 67.9% (95% CI: 53.7, 80.1). These results did not meet the pre-specified success criteria. An appropriate diagnostic cut-off point could not be established to consistently distinguish between GHD and non-GHD patients in the pediatric population.
Geriatric Use
Growth hormone secretion normally decreases with age. Therefore, elderly subjects might require a lower cut-off point for diagnosis of adult growth hormone deficiency. Clinical studies of MACRILEN did not include a sufficient number of subjects aged 65 and over to determine whether elderly patients respond differently from younger subjects.
CONTRAINDICATIONS
None
WARNINGS AND PRECAUTIONS
- QT Prolongation: QT prolongation can lead to development of torsade de pointes-type ventricular tachycardia. Avoid the concomitant use of MACRILEN with drugs that are known to prolong QT interval (5.1 , 7.1 ).
- Potential for False Positive Test Results with Use of Strong CYP3A4 Inducers: Discontinue and washout strong CYP3A4 inducers before testing (5.2 , 7.2 ).
- Potential for False Negative Test Results in Recent Onset Hypothalamic Disease: Consider repeat testing if indicated (5.3 ).
QT Prolongation
MACRILEN causes an increase of about 11 msec in the corrected QT (QTc) interval [see Clinical Pharmacology (12.2 )] . QT prolongation can lead to development of torsade de pointes-type ventricular tachycardia with the risk increasing as the degree of prolongation increases. The concomitant use of MACRILEN with drugs that are known to prolong the QT interval should be avoided [see Dosage and Administration (2.2 ) and Drug Interactions (7.1 )] .
Potential for False Positive Test Results with Use of Strong CYP3A4 Inducers
Concomitant use of strong CYP3A4 inducers with MACRILEN can decrease macimorelin plasma levels significantly and thereby lead to a false positive result [see Drug Interactions (7.2 )] . Strong CYP3A4 inducers should be discontinued and enough time should be given to allow washout of CYP3A4 inducers prior to test administration [see Dosage and Administration (2.2 )].
Potential for False Negative Test Results in Recent Onset Hypothalamic Disease
Adult growth hormone (GH) deficiency caused by a hypothalamic lesion may not be detected early in the disease process. Macimorelin acts downstream from the hypothalamus and macimorelin stimulated release of stored GH reserves from the anterior pituitary could produce a false negative result early when the lesion involves the hypothalamus. Repeat testing may be warranted in this situation.
ADVERSE REACTIONS to report suspected adverse reactions 1-800-332-1088 to report suspected adverse reactions , contact Aeterna Zentaris GmbH at 1-843-900-2332, or FDA at 1‑800-332-1088 or www.fda.gov/medwatch.
Clinical Studies Experience to report suspected adverse reactions 1-800-332-1088 to report suspected adverse reactions , contact Aeterna Zentaris GmbH at 1-843-900-2332, or FDA at 1‑800-332-1088 or www.fda.gov/medwatch.
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trial of another drug and may not reflect the rates observed in practice.
The data in Table 1 are derived from an open-label, randomized, cross-over study that compared the diagnostic performance of MACRILEN to the insulin tolerance test (ITT) for the diagnosis of adult growth hormone deficiency [see Clinical Studies (14 )]. A total of 154 subjects with a high to low pre-test probability of having adult growth hormone deficiency received a single oral dose of 0.5 mg/kg MACRILEN. Out of 154 subjects, 58% were male, 42% female, and 86% of white origin. Median values were for age 41 years (range: 18 – 66 years) and body mass index was 27.5 kg/m 2 (range: 16 – 40 kg/m 2 ). Common adverse reactions presented in Table 1 were adverse reactions that were not present at baseline and occurred during MACRILEN dosing in at least two individuals.
Number of Subjects (n = 154) | Proportion of Subjects (%) | |
Dysgeusia | 7 | 4.5 |
Dizziness | 6 | 3.9 |
Headache | 6 | 3.9 |
Fatigue | 6 | 3.9 |
Nausea | 5 | 3.2 |
Hunger | 5 | 3.2 |
Diarrhea | 3 | 1.9 |
Upper respiratory tract infection | 3 | 1.9 |
Feeling hot | 2 | 1.3 |
Hyperhidrosis | 2 | 1.3 |
Nasopharyngitis | 2 | 1.3 |
Sinus bradycardia | 2 | 1.3 |
The safety of Macrilen was evaluated in 126 pediatric patients. The overall safety profile in the pediatric population was consistent with that observed in adults.
DRUG INTERACTIONS
Drugs that Prolong QT Interval
Co-administration of MACRILEN with drugs that prolong the QT interval (such as antipsychotic medications (e.g., chlorpromazine, haloperidol, thioridazine, ziprasidone), antibiotics (e.g., moxifloxacin), Class 1A (e.g., quinidine, procainamide) and Class III (e.g., amiodarone, sotalol) antiarrhythmic medications or any other medications known to prolong the QT interval) may lead to development of torsade de pointes-type ventricular tachycardia. Avoid concomitant use of MACRILEN with drugs that prolong the QT interval. Sufficient washout time of drugs that are known to prolong the QT interval prior to administration of MACRILEN is recommended [see Dosage and Administration (2.2 ) and Warnings and Precautions (5.1 )] .
Cytochrome P450 (CYP) 3A4 Inducers
Co-administration of a strong CYP3A4 inducer with MACRILEN (e.g., carbamazepine, enzalutamide, mitotane, phenytoin, rifampin, St. John's wort, bosentan, efavirenz, etravirine, modafinil, armodafinil, rufinamide) may reduce the plasma macimorelin concentrations and may lead to false positive test results. Discontinue strong CYP3A4 inducers prior to MACRILEN use. Sufficient washout time of strong CYP3A4 inducers prior to administration of MACRILEN is recommended [see Dosage and Administration (2.2 ) and Warnings and Precautions (5.2 )] .
Drugs Affecting Growth Hormone Release
The following drugs may impact the accuracy of the MACRILEN diagnostic test. Avoid concomitant use of MACRILEN with the following [see Dosage and Administration (2.2 )] :
- Drugs that directly affect the pituitary secretion of growth hormone (such as somatostatin, insulin, glucocorticoids, and cyclooxygenase inhibitors such as aspirin or indomethacin).
- Drugs that may transiently elevate growth hormone concentrations (such as clonidine, levodopa, and insulin).
- Drugs that may blunt the growth hormone response to MACRILEN (such as muscarinic antagonists: atropine, anti-thyroid medication: propylthiouracil, and growth hormone products). Discontinue growth hormone products at least one week before administering the MACRILEN diagnostic test.
Sufficient washout time of drugs affecting growth hormone release prior to administration of MACRILEN is recommended.
DESCRIPTION
MACRILEN for oral solution is macimorelin acetate, a synthetic growth hormone secretagogue receptor agonist. Macimorelin acetate is described chemically as D-Tryptophanamide, 2-methylalanyl-N-[(1R)-1-(formylamino)-2-(1H-indol-3-yl)ethyl]-acetate.
The molecular formula for macimorelin acetate is C 28 H 34 N 6 O 5 with a molecular weight of 534.6 g/mol.
Figure 1: Chemical structure of macimorelin acetate
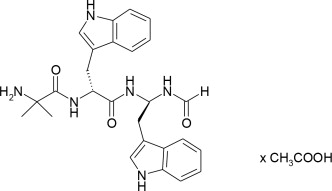
Each aluminum pouch of MACRILEN contains 60 mg of macimorelin, equivalent to 68 mg of macimorelin acetate, and the following inactive ingredients: lactose monohydrate, crospovidone, sodium stearyl fumarate, saccharin sodium and colloidal silicon dioxide.
CLINICAL PHARMACOLOGY
Mechanism of Action
Macimorelin stimulates GH release by activating growth hormone secretagogue receptors present in the pituitary and hypothalamus.
Pharmacodynamics
GH stimulation
Maximum GH levels are observed between 30 to 90 minutes after administration of MACRILEN.
Cardiac electrophysiology
The effects of macimorelin on ECG parameters were investigated in a dedicated Thorough QT study that investigated in a 3-way cross-over design with 60 healthy subjects the effects of a supra-therapeutic dose of macimorelin (2 mg/kg) (4 times the recommended dosage) in comparison with placebo and with moxifloxacin. This study showed a mean baseline- and placebo-adjusted change (upper single-sided 95% confidence interval) in QTcF of 9.6 msec (11.4 msec) at 4 h post-dose, which occurred after the mean maximum macimorelin plasma concentration (0.5 h). A similar increase in the QTcF interval was also observed in a single-ascending dose study, which included three dose levels (0.5 mg/kg, and 1 mg/kg and 2 mg/kg (2 times and 4 times the recommended dosage, respectively). All three dose levels studied showed a similar magnitude of QTcF prolongation in the Thorough QT study, suggesting an absence of dose dependent changes. The mechanism for the observed QTcF prolongation is unknown [see Warnings and Precautions (5.1)] .
Pharmacokinetics
The mean plasma macimorelin concentrations are similar between patients with AGHD and healthy subjects for 1.5 hours following administration of a single oral dose of 0.5 mg macimorelin/kg body weight.
Absorption
The maximum plasma macimorelin concentrations (C max ) were observed between 0.5 hour and 1.5 hours following oral administration of 0.5 mg macimorelin/kg body weight to patients with AGHD under fasting for at least 8 hours. A liquid meal decreased the macimorelin C max and AUC by 55% and 49%, respectively.
Elimination
An in vitro human liver microsomes study showed that CYP3A4 is the major enzyme to metabolize macimorelin.
Macimorelin was eliminated with a mean terminal half-life (T 1/2 ) of 4.1 hours following administration of a single oral dose of 0.5 mg macimorelin/kg body weight in healthy subjects.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Long-term carcinogenesis studies in rodents have not been conducted.
Mutagenesis
Macimorelin did not cause mutations in bacteria under assay conditions with or without metabolic activation. There were also no mutations or clastogenic effects in mouse lymphoma cells with or without metabolic activation.
Impairment of Fertility
No studies have been conducted to assess the effect of macimorelin on fertility.
CLINICAL STUDIES
The diagnostic efficacy of the MACRILEN test was established in a randomized, open-label, single-dose, cross-over study. The objective of the study was to compare the level of agreement between MACRILEN test results and insulin tolerance test (ITT) results in adult patients with different pre-test probability of growth hormone deficiency and healthy control subjects. The four groups of individuals evaluated were:
- Group A : Adults with a high likelihood of growth hormone deficiency (GHD)
- Structural hypothalamic or pituitary lesions and low insulin-like growth factor 1 (IGF-1), and/or
- Three or more pituitary hormone deficiencies and low IGF-1, or
- Childhood onset GHD with structural lesions and low IGF-1.
- Group B : Adults with an intermediate likelihood of GHD
- Eligible subjects not qualifying for either high or low likelihood.
- Group C : Adults with a low likelihood of GHD
- One risk factor for GHD only, such as history of distant traumatic brain injury or one pituitary hormone deficiency only with otherwise normal pituitary function, or
- Isolated idiopathic childhood onset GHD without additional pituitary deficits.
- Group D : Healthy adult controls
- Healthy subjects matching Group A subjects by sex, age ± 5 years, body mass index (BMI ± 2 kg/m 2 ), and estrogen status (females only).
For both the ITT and the MACRILEN test, serum concentrations of growth hormone were measured at 30, 45, 60, and 90 minutes after drug administration. The test was considered positive (i.e., growth hormone deficiency diagnosed) if the maximum serum GH level observed after stimulation was less than the pre-specified cut point value of 2.8 ng/mL for the MACRILEN test or 5.1 ng/mL for the ITT.
The level of negative and positive agreement between the results of the ITT and the MACRILEN test was used to evaluate the performance of the MACRILEN test. In the study, the ITT is used as the benchmark (i.e., a negative ITT indicates absence of disease and a positive ITT indicates presence of disease). Negative agreement is the proportion of subjects with a negative ITT (i.e., those who do not have GHD per the ITT) who also have a negative MACRILEN test. With a high level of negative agreement, the MACRILEN test will not wrongly diagnose an individual without GHD per the ITT as having GHD. Positive agreement is the proportion of subjects with a positive ITT (i.e., those who have GHD per the ITT) who also have a positive MACRILEN test. With a high level of positive agreement, the MACRILEN test will not wrongly diagnose an individual with GHD per the ITT as not having GHD. The agreement measures are defined mathematically below (see Table 2 ).
Insulin Tolerance Test | Total | ||||
+ | |||||
MACRILEN | + | a | b | a+b | Positive Agreement (%)=100% x a/(a+c) |
c | d | c+d | Negative Agreement (%)=100% x d/(b+d) | ||
Total | a+c | b+d | a+b+c+d | Overall Agreement (%)=100% x (a+d)/(a+b+c+d) | |
Results
One hundred and fifty-seven subjects underwent at least one of the two tests in this study, 59% were male, 41% female, and 86% of white origin. The median age was 41 years (range: 18 – 66 years) and body mass index 27.5 kg/m 2 (range: 16 – 40 kg/m 2 ). The study relied on a cross-over design and each participant was to undergo the two diagnostic tests and serve as his or her own control. Data on both tests were available for 140 subjects; 38 (27%) in Group A, 37 (26%) in Group B, 40 (29%) in Group C, and 25 (18%) in Group D. One out of 154 MACRILEN tests (0.6%) performed failed due to a technical error and 27 out of 157 ITTs (17.2%) performed failed because induction of severe hypoglycemia (i.e., the stimulus) could not be achieved.
Two-by-two tables presenting the pre-specified primary analysis results for the ITT and MACRILEN test are shown below for all subjects (Groups A, B, C, and D combined) and for each group separately (see Table 3 ). The estimates for negative and positive agreement between MACRILEN and the ITT in the overall study population were 94% and 74% with lower 95% confidence interval bounds 85% and 63%, respectively. Negative and positive agreement between MACRILEN and the ITT in subjects with intermediate or low risk (Groups B and C) were 93% and 61% with lower 95% confidence interval bounds 80% and 43%, respectively. These results are based on peak GH values (maximum GH concentrations across all measurement timepoints).
All Subjects | Insulin Tolerance Test | Total | Agreement Between | ||||
+ | ITT and MACRILEN | ||||||
MACRILEN | + | 55 | 4 | 59 | Positive | 74% | |
19 | 62 | 81 | Negative | 94% | |||
Total | 74 | 66 | 140 | Overall | 84% | ||
Group A High likelihood of AGHD | Insulin Tolerance Test | Total | |||||
+ | |||||||
MACRILEN | + | 33 | 0 | 33 | Positive | 89% | |
4 | 1 | 5 | Negative | 100% | |||
Total | 37 | 1 | 38 | Overall | 89% | ||
Group B Intermediate likelihood of AGHD | Insulin Tolerance Test | Total | |||||
+ | |||||||
MACRILEN | + | 20 | 1 | 21 | Positive | 67% | |
10 | 6 | 16 | Negative | 86% | |||
Total | 30 | 7 | 37 | Overall | 70% | ||
Group C Low likelihood of AGHD | Insulin Tolerance Test | Total | |||||
+ | |||||||
MACRILEN | + | 2 | 2 | 4 | Positive | 33% | |
4 | 32 | 36 | Negative | 94% | |||
Total | 6 | 34 | 40 | Overall | 85% | ||
Group D Healthy control | Insulin Tolerance Test | Total | |||||
+ | |||||||
MACRILEN | + | 0 | 1 | 1 | Positive | 0% | |
1 | 23 | 24 | Negative | 96% | |||
Total | 1 | 24 | 25 | Overall | 92% | ||
Repeatability was tested in a subset of 34 subjects who underwent two MACRILEN tests. Agreement between the result of the first test and the second test was observed in 31 cases (91.2%).
HOW SUPPLIED/STORAGE AND HANDLING
MACRILEN 60 mg is supplied as white to off-white granules in an aluminum pouch. Each pouch contains 60 mg macimorelin (equivalent to 68 mg macimorelin acetate) that when reconstituted with 120 mL of water provides a 60 mg/120 mL (0.5 mg/mL) macimorelin solution.
MACRILEN is available in boxes containing 1 pouch per box (NDC 0169-1401-01).
Before administration, MACRILEN for oral solution must be reconstituted by a healthcare professional [see Dosage and Administration (2.3 )].
Store pouches under refrigeration at 2-8°C (36-46°F).
The solution must be used within 30 minutes after preparation. Discard unused portion.
Mechanism of Action
Macimorelin stimulates GH release by activating growth hormone secretagogue receptors present in the pituitary and hypothalamus.