Get your patient on Merilog - Insulin Aspart - Szjj injection, Solution (Insulin Aspart-Szjj)
Merilog - Insulin Aspart - Szjj injection, Solution prescribing information
INDICATIONS AND USAGE
MERILOG is indicated to improve glycemic control in adults and pediatric patients with diabetes mellitus.
DOSAGE AND ADMINISTRATION
See Full Prescribing Information for important preparation, administration, and dosage instructions (2.1 , 2.2 , 2.3 , 2.4 , 2.5 ).
- Subcutaneous injection (2.2 ):
- Inject subcutaneously within 5–10 minutes before a meal into the abdominal area, thigh, buttocks or upper arm.
- Rotate injection sites within the same region from one injection to the next to reduce risk of lipodystrophy and localized cutaneous amyloidosis.
- Should generally be used in regimens with an intermediate- or long-acting insulin.
- Individualize and adjust the dosage of MERILOG based on the individual's metabolic needs, blood glucose monitoring results and glycemic control goal (2.3 ).
- Dosage adjustments may be needed with changes in physical activity, changes in meal patterns (i.e., macronutrient content or timing of food intake), changes in renal or hepatic function or during acute illness (2.3 ).
Important Preparation and Administration Instructions
- Always check insulin labels before administration [see Warnings and Precautions (5.4) ].
- Inspect MERILOG visually before use. It should appear clear and colorless. Do not use MERILOG if particulate matter or coloration is seen.
- Use MERILOG SoloStar prefilled pen with caution in patients with visual impairment who may rely on audible clicks to dial their dose.
Preparation and Administration Instructions for the Approved Routes of Administration
Subcutaneous Injection
- Inject MERILOG subcutaneously within 5–10 minutes before a meal into the abdominal area, thigh, buttocks or upper arm.
- Rotate injection sites within the same region from one injection to the next to reduce the risk of lipodystrophy and localized cutaneous amyloidosis. Do not inject into areas of lipodystrophy or localized cutaneous amyloidosis [see Warnings and Precautions (5.2) and Adverse Reactions (6.1 , 6.3) ].
- The MERILOG SoloStar prefilled pen dials in 1-unit increments.
- Generally use MERILOG (administered by subcutaneous injection) in regimens with an intermediate- or long-acting insulin.
Dosage Recommendations
- Individualize the dosage of MERILOG based on the patient's metabolic needs, blood glucose monitoring results and glycemic control goal.
- Dosage adjustments may be needed with changes in physical activity, changes in meal patterns (i.e., macronutrient content or timing of food intake), changes in renal or hepatic function or during acute illness [see Warnings and Precautions (5.2 , 5.3 ) and Use in Specific Populations (8.6 , 8.7 )] .
- When switching from another insulin to MERILOG, a different dosage of MERILOG may be needed [see Warnings and Precautions (5.2) ].
- During changes to a patient's insulin regimen, increase the frequency of blood glucose monitoring [see Warnings and Precautions (5.2) ] .
Dosage Modifications for Drug Interactions
- Dosage modification may be needed when MERILOG is used concomitantly with certain drugs [see Drug Interactions (7) ] .
Instructions for Mixing MERILOG with Other Insulins
Do notmix MERILOG with any other insulin.
DOSAGE FORMS AND STRENGTHS
Injection: 100 units/mL (U-100) is a clear and colorless solution available as:
- 10 mL multiple-dose vial
- 3 mL single-patient-use MERILOG SoloStar ® prefilled pen
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
Available information from published randomized controlled trials with insulin aspart products use during the second trimester of pregnancy have not reported an association with insulin aspart products and major birth defects or adverse maternal or fetal outcomes [see Data ] . There are risks to the mother and fetus associated with poorly controlled diabetes in pregnancy [see Clinical Considerations ] .
In animal reproduction studies, administration of subcutaneous insulin aspart to pregnant rats and rabbits during the period of organogenesis did not cause adverse developmental effects at exposures 8-times and equal to the human subcutaneous dose of 1 unit/kg/day, respectively. Pre- and post-implantation losses and visceral/skeletal abnormalities were seen at higher exposures, which are considered secondary to maternal hypoglycemia. These effects were similar to those observed in rats administered regular human insulin [see Data ] .
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively. The estimated background risk of major birth defects is 6 to 10% in women with pre-gestational diabetes with a periconceptual HbA 1c >7% and has been reported to be as high as 20 to 25% in women with a periconceptual HbA 1c >10%. The estimated background risk of miscarriage for the indicated population is unknown.
Clinical Considerations
Disease-Associated Maternal and/or Embryo-Fetal Risk
Poorly controlled diabetes in pregnancy increases the maternal risk for diabetic ketoacidosis, preeclampsia, spontaneous abortions, preterm delivery, and delivery complications. Poorly controlled diabetes increases the fetal risk for major birth defects, stillbirth, and macrosomia related morbidity.
Data
Human Data
Published data from 5 randomized controlled trials of 441 pregnant women with diabetes mellitus treated with insulin aspart products during the late 2 nd trimester of pregnancy did not identify an association of insulin aspart products with major birth defects or adverse maternal or fetal outcomes. However, these studies cannot definitely establish the absence of any risk because of methodological limitations, including a variable duration of treatment and small size of the majority of the trials.
Animal Data
Fertility, embryo-fetal and pre- and postnatal development studies have been performed with insulin aspart and regular human insulin in rats and rabbits. In a combined fertility and embryo-fetal development study in rats, insulin aspart was administered before mating, during mating, and throughout pregnancy. Further, in a pre- and postnatal development study insulin aspart was given throughout pregnancy and during lactation to rats. In an embryo-fetal development study insulin aspart was given to female rabbits during organogenesis. The effects of insulin aspart did not differ from those observed with subcutaneous regular human insulin. Insulin aspart, like human insulin, caused pre- and post-implantation losses and visceral/skeletal abnormalities in rats at a dose of 200 units/kg/day (approximately 32 times the human subcutaneous dose of 1 unit/kg/day, based on human exposure equivalents) and in rabbits at a dose of 10 units/kg/day (approximately three times the human subcutaneous dose of 1 unit/kg/day, based on human exposure equivalents). No significant effects were observed in rats at a dose of 50 units/kg/day and in rabbits at a dose of 3 units/kg/day. These doses are approximately 8 times the human subcutaneous dose of 1 unit/kg/day for rats and equal to the human subcutaneous dose of 1 unit/kg/day for rabbits, based on human exposure equivalents. The effects are considered secondary to maternal hypoglycemia.
Lactation
Risk Summary
There are no data on the presence of insulin aspart products in human milk, the effects on the breastfed infant, or the effect on milk production. One small published study reported that exogenous insulin, including insulin aspart, was present in human milk. However, there is insufficient information to determine the effects of insulin aspart products on the breastfed infant. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for MERILOG, and any potential adverse effects on the breastfed infant from MERILOG, or from the underlying maternal condition.
Pediatric Use
The safety and effectiveness of MERILOG to improve glycemic control have been established in pediatric patients with diabetes mellitus. Use of MERILOG for this indication is supported by evidence from an adequate and well-controlled study of insulin aspart in 283 pediatric patients with type 1 diabetes mellitus aged 6 to 18 years and from studies in adults with diabetes mellitus [see Adverse Reactions (6.1) , Clinical Pharmacology (12.3) , and Clinical Studies (14) ] .
Geriatric Use
Of the total number of patients (n=1,375) treated with insulin aspart in 3 controlled clinical studies, 2.6% (n=36) were 65 years of age or over. One-half of these patients had type 1 diabetes (18/1285) and the other half had type 2 diabetes (18/90). The HbA 1c response to insulin aspart, as compared to regular human insulin, did not differ by age.
Renal Impairment
Patients with renal impairment may be at increased risk of hypoglycemia and may require more frequent MERILOG dose adjustment and more frequent blood glucose monitoring [see Warnings and Precautions (5.3) and Clinical Pharmacology (12.3) ] .
Hepatic Impairment
Patients with hepatic impairment may be at increased risk of hypoglycemia and may require more frequent MERILOG dose adjustment and more frequent blood glucose monitoring [see Warnings and Precautions (5.3) and Clinical Pharmacology (12.3) ] .
CONTRAINDICATIONS
MERILOG is contraindicated:
- During episodes of hypoglycemia [see Warnings and Precautions (5.3) ].
- In patients with hypersensitivity to insulin aspart products or any of the excipients in MERILOG [see Warnings and Precautions (5.5) ].
WARNINGS AND PRECAUTIONS
- Never share a MERILOG SoloStar prefilled pen between patients, even if the needle is changed (5.1 ).
- Hyperglycemia or hypoglycemia with changes in insulin regimen: Make changes to a patient's insulin regimen (e.g., insulin strength, manufacturer, type, injection site or method of administration) under close medical supervision with increased frequency of blood glucose monitoring (5.2 ).
- Hypoglycemia: May be life-threatening. Increase frequency of glucose monitoring with changes to: insulin dosage, concomitantly administered glucose lowering medications, meal pattern, physical activity; and in patients with renal or hepatic impairments and hypoglycemia unawareness (5.3 ).
- Medication Errors: Accidental mix-ups between insulin products can occur. Instruct patients to check insulin labels before injection (5.4 ).
- Hypersensitivity reactions: Severe, life-threatening, generalized allergy, including anaphylaxis, may occur. Discontinue MERILOG, treat, and monitor, if indicated (5.5 ).
- Hypokalemia: May be life-threatening. Monitor potassium levels in patients at risk of hypokalemia and treat if indicated (5.6 ).
- Fluid retention and heart failure with concomitant use of thiazolidinediones (TZDs): Observe for signs and symptoms of heart failure; consider dosage reduction or discontinuation if heart failure occurs (5.7 ).
Never Share a MERILOG SoloStar Prefilled Pen Between Patients
MERILOG SoloStar prefilled pen should never be shared between patients, even if the needle is changed. Patients using MERILOG vials must never share needles or syringes with another person. Sharing poses a risk for transmission of blood-borne pathogens.
Hyperglycemia or Hypoglycemia with Changes in Insulin Regimen
Changes in an insulin regimen (e.g., insulin strength, manufacturer, type, injection site or method of administration) may affect glycemic control and predispose to hypoglycemia [see Warnings and Precautions (5.3) ] or hyperglycemia. Repeated insulin injections into areas of lipodystrophy or localized cutaneous amyloidosis have been reported to result in hyperglycemia; and a sudden change in the injection site (to an unaffected area) has been reported to result in hypoglycemia [see Adverse Reactions (6.1 , 6.3) ] .
Make any changes to a patient's insulin regimen under close medical supervision with increased frequency of blood glucose monitoring. Advise patients who have repeatedly injected into areas of lipodystrophy or localized cutaneous amyloidosis to change the injection site to unaffected areas and closely monitor for hypoglycemia. For patients with type 2 diabetes, dosage adjustments of concomitant anti-diabetic products may be needed.
Hypoglycemia
Hypoglycemia is the most common adverse reaction of all insulins, including insulin aspart products. Severe hypoglycemia can cause seizures, may lead to unconsciousness, may be life threatening or cause death. Hypoglycemia can impair concentration ability and reaction time; this may place an individual and others at risk in situations where these abilities are important (e.g., driving or operating other machinery).
Hypoglycemia can happen suddenly and symptoms may differ in each individual and change over time in the same individual. Symptomatic awareness of hypoglycemia may be less pronounced in patients with longstanding diabetes in patients with diabetic nerve disease, in patients using medications that block the sympathetic nervous system (e.g., beta-blockers) [see Drug Interactions (7) ] , or in patients who experience recurrent hypoglycemia.
Risk Factors for Hypoglycemia
The risk of hypoglycemia after an injection is related to the duration of action of the insulin and, in general, is highest when the glucose lowering effect of the insulin is maximal. As with all insulins, the glucose lowering effect time course of insulin aspart products may vary in different individuals or at different times in the same individual and depends on many conditions, including the area of injection as well as the injection site blood supply and temperature [see Clinical Pharmacology (12.2) ] . Other factors which may increase the risk of hypoglycemia include changes in meal pattern (e.g., macronutrient content or timing of meals), changes in level of physical activity, or changes to concomitantly administered medication [see Drug Interactions (7) ] . Patients with renal or hepatic impairment may be at higher risk of hypoglycemia [see Use in Specific Populations (8.6 , 8.7 )] .
Risk Mitigation Strategies for Hypoglycemia
Patients and caregivers must be educated to recognize and manage hypoglycemia. Self-monitoring of blood glucose plays an essential role in the prevention and management of hypoglycemia; increased frequency of blood glucose monitoring is recommended. In patients at higher risk for hypoglycemia and patients who have reduced symptomatic awareness of hypoglycemia, increased frequency of blood glucose monitoring is recommended.
Hypoglycemia Due to Medication Errors
Accidental mix-ups between insulin products have been reported. To avoid medication errors between MERILOG and other insulins, instruct patients to always check the insulin label before each injection.
Hypersensitivity Reactions
Severe, life-threatening, generalized allergy, including anaphylaxis, can occur with insulins, including insulin aspart products. If hypersensitivity reactions occur, discontinue MERILOG; treat per standard of care and monitor until symptoms and signs resolve [see Adverse Reactions (6) ] . MERILOG is contraindicated in patients who have had hypersensitivity reactions to insulin aspart products or any of the excipients in MERILOG [see Contraindications (4) ] .
Hypokalemia
All insulins, including insulin aspart products, can cause a shift in potassium from the extracellular to intracellular space, possibly leading to hypokalemia. Untreated hypokalemia may cause respiratory paralysis, ventricular arrhythmia, and death. Monitor potassium levels in patients at risk for hypokalemia if indicated (e.g., patients using potassium-lowering medications, patients taking medications sensitive to serum potassium concentration).
Fluid Retention and Heart Failure with Concomitant Use of PPAR-gamma Agonists
Thiazolidinediones (TZDs), which are peroxisome proliferator-activated receptor (PPAR)-gamma agonists, can cause dose-related fluid retention, particularly when used in combination with insulin. Fluid retention may lead to or exacerbate heart failure. Patients treated with insulin, including MERILOG, and a PPAR-gamma agonist should be observed for signs and symptoms of heart failure. If heart failure develops, it should be managed according to current standards of care, and discontinuation or dose reduction of the PPAR-gamma agonist must be considered.
ADVERSE REACTIONS
The following adverse reactions are also discussed elsewhere:
- Hypoglycemia [see Warnings and Precautions (5.3) ]
- Hypoglycemia Due to Medication Errors [see Warnings and Precautions (5.4) ]
- Hypersensitivity Reactions [see Warnings and Precautions (5.5) ]
- Hypokalemia [see Warnings and Precautions (5.6) ]
Clinical Trials Experience
Because clinical trials are conducted under widely varying designs, the adverse reaction rates reported in one clinical trial may not be easily compared to those rates reported in another clinical trial, and may not reflect the rates actually observed in clinical practice. The safety of insulin aspart was evaluated in two treat-to-target trials of 6 months duration, conducted in patients with type 1 diabetes or type 2 diabetes [see Clinical Studies (14) ] .
The data in Table 1 reflect the exposure of 596 patients with type 1 diabetes to insulin aspart in one clinical trial with a mean exposure duration to insulin aspart of 24 weeks. The mean age was 39 years. Fifty-one percent were male, 94% were Caucasian, 2% were Black and 4% were other races. The mean body mass index (BMI) was 25.6 kg/m 2 . The mean duration of diabetes was 15.7 years and the mean HbA 1c at baseline was 7.9%.
The data in Table 2 reflect the exposure of 91 patients with type 2 diabetes to insulin aspart in one clinical trial with a mean exposure duration to insulin aspart of 24 weeks. The mean age was 57 years. Sixty-three percent were male, 76% were Caucasian, 9% were Black and 15% were other races. The mean BMI was 29.7 kg/m 2 . The mean duration of diabetes was 12.7 years and the mean HbA 1c at baseline was 8.1%.
Common adverse reactions were defined as events that occurred in ≥5%, excluding hypoglycemia, of the population studied. Common adverse events that occurred at the same rate or greater for insulin aspart-treated patients than in comparator-treated patients during clinical trials in patients with type 1 diabetes mellitus and type 2 diabetes mellitus (other than hypoglycemia) are listed in Table 1 and Table 2, respectively.
| Insulin aspart + NPH (%) (n= 596) | Regular Human Insulin + NPH (%) (n= 286) | |
|---|---|---|
| Headache | 12 | 10 |
| Injury accidental | 11 | 10 |
| Nausea | 7 | 5 |
| Diarrhea | 5 | 3 |
| Insulin aspart + NPH (%) (n= 91) | Human Regular Insulin + NPH (%) (n= 91) | |
|---|---|---|
| Hyporeflexia | 11 | 7 |
| Onychomycosis | 10 | 5 |
| Sensory disturbance | 9 | 7 |
| Urinary tract infection | 8 | 7 |
| Chest pain | 5 | 3 |
| Headache | 5 | 3 |
| Skin disorder | 5 | 2 |
| Abdominal pain | 5 | 1 |
| Sinusitis | 5 | 1 |
Severe Hypoglycemia
Hypoglycemia is the most commonly observed adverse reaction in patients using insulin, including insulin aspart products [see Warnings and Precautions (5.3) ] . The rates of reported hypoglycemia depend on the definition of hypoglycemia used, diabetes type, insulin dose, intensity of glucose control, background therapies, and other intrinsic and extrinsic patient factors. For these reasons, comparing rates of hypoglycemia in clinical trials for insulin aspart with the incidence of hypoglycemia for other products may be misleading and also, may not be representative of hypoglycemia rates that will occur in clinical practice.
Severe hypoglycemia was defined as hypoglycemia associated with central nervous system symptoms and requiring the intervention of another person or hospitalization. The incidence of severe hypoglycemia in:
- Adult and pediatric patients with type 1 diabetes mellitus who received subcutaneous insulin aspart was 17% at 24 weeks and 6% at 24 weeks, respectively [see Clinical Studies (14) ] .
- Adult patients with type 2 diabetes mellitus who received subcutaneous insulin aspart was 10% at 24 weeks.
Allergic Reactions
Some patients taking insulin, including insulin aspart products have experienced erythema, local edema, and pruritus at the site of injection. These conditions were usually self-limiting. Severe cases of generalized allergy (anaphylaxis) have been reported.
Adverse Reactions Associated with Insulin Initiation and Glucose Control Intensification
Intensification or rapid improvement in glucose control has been associated with a transitory, reversible ophthalmologic refraction disorder, worsening of diabetic retinopathy, and acute painful peripheral neuropathy. However, long-term glycemic control decreases the risk of diabetic retinopathy and neuropathy.
Lipodystrophy
Administration of insulin, including insulin aspart products subcutaneously, has resulted in lipoatrophy (depression in the skin) or lipohypertrophy (enlargement or thickening of tissue) in some patients [see Dosage and Administration (2.2) ] .
Peripheral Edema
Insulins, including insulin aspart products, may cause sodium retention and edema, particularly if previously poor metabolic control is improved by intensified insulin therapy.
Weight Gain
Weight gain has occurred with insulins, including insulin aspart products, and has been attributed to the anabolic effects of insulin and the decrease in glucosuria.
Immunogenicity
As with all therapeutic proteins, there is potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies in the studies described below with the incidence of antibodies in other studies or to other insulin aspart products may be misleading.
In a 6-month study with a 6-month extension in adult subjects with type 1 diabetes, 99.8% of patients who received insulin aspart were positive for anti-insulin antibodies (AIA) at least once during the study, including 97.2% that were positive at baseline. A total of 92.1% of patients who received insulin aspart were positive for anti-drug antibodies (ADA) at least once during the study, including 64.6% that were positive at baseline.
In a phase 3 type 1 diabetes clinical trial of insulin aspart, initial increase in titers of antibodies to insulin, followed by a decrease to baseline values, was observed in regular human insulin and insulin aspart treatment groups with similar incidences. These antibodies did not cause deterioration in glycemic control or necessitate increases in insulin dose.
Postmarketing Experience
The following adverse reactions have been identified during post-approval use of insulin aspart products. Because these adverse reactions are reported voluntarily from a population of uncertain size, it is generally not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Medication errors have been reported in which other insulins have been accidentally substituted for insulin aspart products.
Localized cutaneous amyloidosis at the injection site has occurred with insulin aspart products. Hyperglycemia has been reported with repeated insulin injections into areas of localized cutaneous amyloidosis; hypoglycemia has been reported with a sudden change to an unaffected injection site.
DRUG INTERACTIONS
The table below presents clinically significant drug interactions with MERILOG.
| Drugs That May Increase the Risk of Hypoglycemia | |
|---|---|
| Drugs: | Antidiabetic agents, ACE inhibitors, angiotensin II receptor blocking agents, disopyramide, fibrates, fluoxetine, monoamine oxidase inhibitors, pentoxifylline, pramlintide, salicylates, somatostatin analog (e.g., octreotide), and sulfonamide antibiotics. |
| Intervention: | Dose adjustment and increased frequency of glucose monitoring may be required when MERILOG is concomitantly administered with these drugs. |
| Drugs That May Decrease the Blood Glucose Lowering Effect of MERILOG | |
| Drugs: | Atypical antipsychotics (e.g., olanzapine and clozapine), corticosteroids, danazol, diuretics, estrogens, glucagon, isoniazid, niacin, oral contraceptives, phenothiazines, progestogens (e.g., in oral contraceptives), protease inhibitors, somatropin, sympathomimetic agents (e.g., albuterol, epinephrine, terbutaline), and thyroid hormones. |
| Intervention: | Dose adjustment and increased frequency of glucose monitoring may be required when MERILOG is concomitantly administered with these drugs. |
| Drugs That May Increase or Decrease the Blood Glucose Lowering Effect of MERILOG | |
| Drugs: | Alcohol, beta-blockers, clonidine, and lithium salts. Pentamidine may cause hypoglycemia, which may sometimes be followed by hyperglycemia. Pentamidine may cause hypoglycemia, which may sometimes be followed by hyperglycemia. |
| Intervention: | Dose adjustment and increased frequency of glucose monitoring may be required when MERILOG is concomitantly administered with these drugs. |
| Drugs That May Blunt Signs and Symptoms of Hypoglycemia | |
| Drugs: | Beta-blockers, clonidine, guanethidine and reserpine |
| Intervention: | Increased frequency of glucose monitoring may be required when MERILOG is concomitantly administered with these drugs. |
DESCRIPTION
Insulin aspart-szjj is a rapid-acting human insulin analog homologous with regular human insulin with the exception of a single substitution of the amino acid proline by aspartic acid in position B28, and is produced by recombinant DNA technology utilizing Escherichia coli . Insulin aspart-szjj has a molecular weight of 5825.8 Da.
MERILOG (insulin aspart-szjj) injection is a sterile, clear, and colorless solution for subcutaneous use. Each mL contains 100 units of insulin aspart-szjj and the inactive ingredients: 1.72 mg metacresol, 1.50 mg phenol, 0.02 mg polysorbate 20, 6.80 mg sodium chloride, 0.04 mg zinc chloride and Water for Injection, USP. MERILOG has a pH of 7.0–7.8. Hydrochloric acid and/or sodium hydroxide may be added to adjust pH.
CLINICAL PHARMACOLOGY
Mechanism of Action
The primary activity of insulin, including insulin aspart products is the regulation of glucose metabolism. Insulin and its analogs lower blood glucose by stimulating peripheral glucose uptake, especially by skeletal muscle and fat, and by inhibiting hepatic glucose production. Insulin inhibits lipolysis and proteolysis, and enhances protein synthesis.
Pharmacodynamics
Pharmacodynamics of Insulin Aspart After Subcutaneous Administration
The pharmacodynamic profile of insulin aspart given subcutaneously in 22 patients with type 1 diabetes is shown in Figure 1. The maximum glucose-lowering effect of insulin aspart occurred between 1 and 3 hours after subcutaneous injection (0.15 units/kg). The duration of action for insulin aspart is 3 to 5 hours. The time course of action of insulin and insulin analogs such as insulin aspart products may vary considerably in different individuals or within the same individual. The parameters of insulin aspart activity (time of onset, peak time and duration) as designated in Figure 1 should be considered only as general guidelines. The rate of insulin absorption and onset of activity is affected by the site of injection, exercise, and other variables [see Warnings and Precautions (5.3) ] .
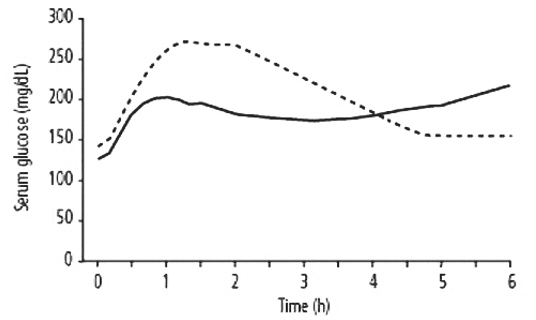
Figure 1. Serial mean serum glucose collected up to 6 hours following a single 0.15 units/kg pre-meal dose of insulin aspart (solid curve) or regular human insulin (hatched curve) injected immediately before a meal in 22 patients with type 1 diabetes.
Pharmacokinetics
Pharmacokinetics of subcutaneous administration of insulin aspart is presented below.
Absorption and Bioavailability
In studies in healthy volunteers (total n=107) and patients with type 1 diabetes (total n=40), the median time to maximum concentration of insulin aspart in these trials was 40 to 50 minutes versus 80 to 120 minutes, for regular human insulin respectively.
The relative bioavailability of insulin aspart (0.15 units/kg) compared to regular human insulin indicates that the two insulins are absorbed to a similar extent.
In a clinical trial in patients with type 1 diabetes, insulin aspart and regular human insulin, both administered subcutaneously at a dose of 0.15 units/kg body weight, reached mean maximum concentrations of 82 and 36 mU/L, respectively.
Distribution
Insulin aspart has a low binding affinity to plasma proteins (<10%), similar to that seen with regular human insulin.
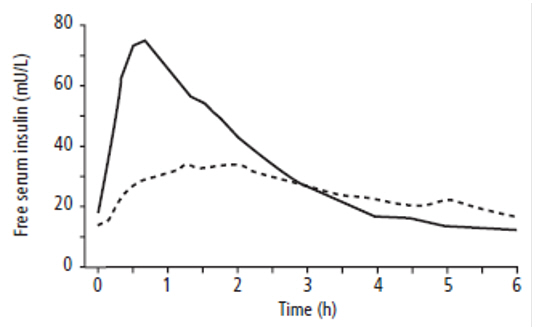
Figure 2. Serial mean serum free insulin concentration collected up to 6 hours following a single 0.15 units/kg pre-meal dose of insulin aspart (solid curve) or regular human insulin (hatched curve) injected immediately before a meal in 22 patients with type 1 diabetes.
Metabolism and Elimination
After subcutaneous administration in normal male volunteers (n=24), insulin aspart was eliminated with an average apparent half-life of 81 minutes.
Specific Populations
Pediatric Patients : The pharmacokinetic and pharmacodynamic properties of insulin aspart and regular human insulin were evaluated in a single dose study in 18 pediatric patients with type 1 diabetes in 2 age groups: 6–12 years, n=9 and 13–17 years (Tanner grade ≥2), n=9. The relative differences in pharmacokinetics and pharmacodynamics in the pediatric patients with type 1 diabetes in both age groups between insulin aspart and regular human insulin were similar to those in healthy adult subjects and adults with type 1 diabetes.
Geriatric Patients : The pharmacokinetic and pharmacodynamic properties of insulin aspart and regular human insulin were investigated in a single dose study in 18 subjects with type 2 diabetes who were ≥65 years of age. The relative differences in pharmacokinetics and pharmacodynamics in geriatric patients with type 2 diabetes between insulin aspart and regular human insulin were similar to those in younger adults.
Male and Female Patients : In healthy volunteers given a single subcutaneous dose of insulin aspart 0.06 units/kg, no difference in insulin aspart levels was seen between males and females based on comparison of AUC (0–10h) or C max .
Obese Patients : A single subcutaneous dose of 0.1 units/kg insulin aspart was administered in a study of 23 patients with type 1 diabetes and a wide range of body mass index (BMI, 22–39 kg/m 2 ). The pharmacokinetic parameters, AUC and C max , of insulin aspart were generally unaffected by BMI in the different groups – BMI 19–23 kg/m 2 (n=4); BMI 23–27 kg/m 2 (n=7); BMI 27–32 kg/m 2 (n=6) and BMI >32 kg/m 2 (n=6). Clearance of insulin aspart was reduced by 28% in patients with BMI >32 kg/m 2 compared to patients with BMI <23 kg/m 2 .
Patients with Renal Impairment : A single subcutaneous dose of 0.08 units/kg insulin aspart was administered in a study to subjects with either normal renal function (n=6) creatinine clearance (CLcr) (>80 ml/min) or mild (n=7; CLcr=50–80 ml/min), moderate (n=3; CLcr=30–50 ml/min) or severe (but not requiring hemodialysis) (n=2; CLcr = <30 ml/min) renal impairment. In this study, there was no apparent effect of creatinine clearance values on AUC and C max of insulin aspart.
Patients with Hepatic Impairment : A single subcutaneous dose of 0.06 units/kg insulin aspart was administered in an open-label, single-dose study of 24 subjects (n=6/group) with different degree of hepatic impairment (mild, moderate and severe) having Child-Pugh Scores ranging from 0 (healthy volunteers) to 12 (severe hepatic impairment). In this study, there was no correlation between the degree of hepatic impairment and any insulin aspart pharmacokinetic parameter.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Standard 2-year carcinogenicity studies in animals have not been performed to evaluate the carcinogenic potential of insulin aspart products. In 52-week studies, Sprague-Dawley rats were dosed subcutaneously with insulin aspart at 10, 50, and 200 units/kg/day (approximately 2, 8, and 32 times the human subcutaneous dose of 1.0 units/kg/day, based on units/body surface area, respectively). At a dose of 200 units/kg/day, insulin aspart increased the incidence of mammary gland tumors in females when compared to untreated controls. The relevance of these findings to humans is unknown.
Insulin aspart was not genotoxic in the following tests: Ames test, mouse lymphoma cell forward gene mutation test, human peripheral blood lymphocyte chromosome aberration test, in vivo micronucleus test in mice, and in ex vivo UDS test in rat liver hepatocytes.
In fertility studies in male and female rats, at subcutaneous doses up to 200 units/kg/day (approximately 32 times the human subcutaneous dose, based on units/body surface area), no direct adverse effects on male and female fertility, or general reproductive performance of animals was observed.
Animal Toxicology and/or Pharmacology
In standard biological assays in mice and rabbits, one unit of insulin aspart has the same glucose-lowering effect as one unit of regular human insulin.
CLINICAL STUDIES
Overview of Clinical Studies
The safety and effectiveness of subcutaneous insulin aspart were compared to regular human insulin in 596 type 1 diabetes adult, 187 pediatric type 1 diabetes, and 91 adult type 2 diabetes patients using NPH as basal insulin (see Tables 3 , 4 , 5 ). The reduction in glycated hemoglobin (HbA 1c ) was similar to regular human insulin.
Clinical Studies in Adult and Pediatric Patients with Type 1 Diabetes with Subcutaneous Injections
Type 1 Diabetes - Adults (see Table 3 )
Two 24-week, open-label, active-controlled studies were conducted to compare the safety and efficacy of insulin aspart to regular human insulin injection in adult patients with type 1 diabetes. Because the two study designs and results were similar, data are shown for only one study (see Table 3 ).
The mean age of the trial population was 39 years and mean duration of diabetes was 15.7 years. Fifty-one percent were male. Ninety-four percent were Caucasian, 2% were Black and 4% were Other. The mean BMI was approximately 25.6 kg/m 2 .
Insulin aspart was administered by subcutaneous injection immediately prior to meals and regular human insulin was administered by subcutaneous injection 30 minutes before meals. NPH insulin was administered as the basal insulin in either single or divided daily doses. Changes in HbA 1c were comparable for the two treatment regimens in this study (Table 3).
| Insulin aspart + NPH (n=596) | Regular Human Insulin + NPH (n=286) | |
|---|---|---|
| Baseline HbA 1c (%) Values are Mean ± SD | 7.9 ± 1.1 | 8.0 ± 1.2 |
| Change from Baseline HbA 1c (%) | -0.1 ± 0.8 | 0.0 ± 0.8 |
| Treatment Difference in HbA 1c , Mean (95% confidence interval) | -0.2 (-0.3, -0.1) | |
Type 1 Diabetes – Pediatric (see Table 4 )
The efficacy of insulin aspart to improve glycemic control in pediatric patients with type 1 diabetes mellitus is based on an adequate and well-controlled trial of regular human insulin in pediatric patients with type 1 diabetes mellitus (Table 4). This 24-week, parallel-group study of pediatric patients with type 1 diabetes (n=283), aged 6 to 18 years, compared two subcutaneous multiple-dose treatment regimens: insulin aspart (n=187) or regular human insulin (n=96). NPH insulin was administered as the basal insulin. Similar effects on HbA 1c were observed in both treatment groups (Table 4).
Subcutaneous administration of insulin aspart and regular human insulin have also been compared in pediatric patients with type 1 diabetes (n=26) aged 2 to 6 years with similar effects on HbA 1c .
| Insulin aspart + NPH (n=187) | Regular Human Insulin + NPH (n=96) | |
|---|---|---|
| Baseline HbA 1c (%) Values are Mean ± SD | 8.3 ± 1.2 | 8.3 ± 1.3 |
| Change from Baseline HbA 1c (%) | 0.1 ± 1.0 | 0.1 ± 1.1 |
| Treatment Difference in HbA 1c , Mean (95% confidence interval) | -0.2 (-0.5, 0.1) | |
Clinical Studies in Adults with Type 2 Diabetes with Subcutaneous Injections
Type 2 Diabetes - Adults (see Table 5 )
One six-month, open-label, active-controlled study was conducted to compare the safety and efficacy of insulin aspart to regular human insulin in patients with type 2 diabetes (Table 5).
The mean age of the trial population was 56.6 years and mean duration of diabetes was 12.7 years. Sixty-three percent were male. Seventy-six percent were Caucasian, 9% were Black and 15% were Other. The mean BMI was approximately 29.7 kg/m 2 .
Insulin aspart was administered by subcutaneous injection immediately prior to meals and regular human insulin was administered by subcutaneous injection 30 minutes before meals. NPH insulin was administered as the basal insulin in either single or divided daily doses. Changes in HbA 1c were comparable for the two treatment regimens.
| Insulin aspart + NPH (n=90) | Regular Human Insulin + NPH (n=86) | |
|---|---|---|
| Baseline HbA 1c (%) Values are Mean ± SD | 8.1 ± 1.2 | 7.8 ± 1.1 |
| Change from Baseline HbA 1c (%) | -0.3 ± 1.0 | -0.1 ± 0.8 |
| Treatment Difference in HbA 1c , Mean (95% confidence interval) | -0.1 (-0.4, 0.1) | |
HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
MERILOG (insulin aspart-szjj) injection 100 units/mL (U-100) is available as a clear and colorless solution in:
| Dosage Unit | NDC # |
|---|---|
| One 10 mL multiple-dose vial per carton | NDC 0024-5927-00 |
| Five 3 mL single-patient-use SoloStar prefilled pens per carton | NDC 0024-5928-05 |
The MERILOG SoloStar prefilled pen dials in 1-unit increments.
Needles are not included in MERILOG SoloStar packs. Only use needles that are compatible for use with MERILOG SoloStar which are sold separately, including needles from Becton, Dickinson and company (BD) (such as BD Ultra-Fine ® ), Ypsomed (such as Clickfine ® ), and Owen Mumford (such as Unifine ® Pentips ® ).
Recommended Storage
Dispense in the original sealed carton with the enclosed Instructions for Use.
Store unused MERILOG in a refrigerator between 2°C to 8°C (36°F to 46°F). Do not freeze MERILOG and do not use MERILOG if it has been frozen. Do not expose MERILOG to excessive heat or light.
Do notwithdraw MERILOG into a syringe and store for later use.
Always remove and discard the needle after each injection from the MERILOG SoloStar prefilled pen and store without a needle attached.
The storage conditions are summarized in the following table:
| MERILOG presentation | Not in-use (unopened) Room Temperature (up to 30°C [86°F]) | Not in-use (unopened) Refrigerated (2°C to 8°C [36°F to 46°F]) | In-use (opened) Room Temperature (up to 30°C [86°F]) |
|---|---|---|---|
| 10 mL multiple-dose vial | 28 days | Until expiration date | 28 days (refrigerated/room temperature) |
| 3 mL single-patient-use SoloStar prefilled pen | 28 days | Until expiration date | 28 days (Do not refrigerate) |
INSTRUCTIONS FOR USE MERILOG™ [mer-ih-lawg] (insulin aspart-szjj) injection, for subcutaneous use 10 mL multiple-dose vial: 100 units/mL (U-100)
This Instructions for Use contains information on how to inject MERILOG.
Read this Instructions for Use before you start taking MERILOG and each time you get a new MERILOG vial. There may be new information. This information does not take the place of talking to your healthcare provider about your medical condition or your treatment.
Do not share your MERILOG syringes with other people, even if the needle has been changed. You may give other people a serious infection, or get a serious infection from them.
Supplies needed to give your injection
- a MERILOG 10 mL vial
- a U-100 insulin syringe and needle
- 2 alcohol swabs
- 1 sharps container for throwing away used needles and syringes. See " Disposing of used needles and syringes " at the end of these instructions.
Preparing your MERILOG dose
- Wash your hands with soap and water or with alcohol.
- Check the MERILOG label to make sure you are taking the right type of insulin. This is especially important if you use more than 1 type of insulin.
- Check that the insulin is clear and colorless. Do not use the vial if the insulin looks cloudy, colored or contains particles.
- Do not use MERILOG after the expiration date stamped on the label or 28 days after you first use it.
- Always use a syringe that is marked for U-100 insulin . If you use a syringe other than a U-100 insulin syringe, you may get the wrong dose of insulin.
- Always use a new syringe or needle for each injection to help maintain sterility and prevent blocked needles. Do not reuse or share your syringes or needles with other people. You may give other people a serious infection or get a serious infection from them.
Need help?
If you have any questions about your vial or about diabetes, ask your healthcare provider, or call sanofi-aventis at 1-800-633-1610.
Step 1:
If you are using a new vial, remove the protective cap. Do not remove the stopper (see Figure A ).
 ( Figure A )
( Figure A )
Step 2:
Wipe the top of the vial with an alcohol swab. You do not have to shake the vial of MERILOG before use (see Figure B ).
 ( Figure B )
( Figure B )
Step 3:
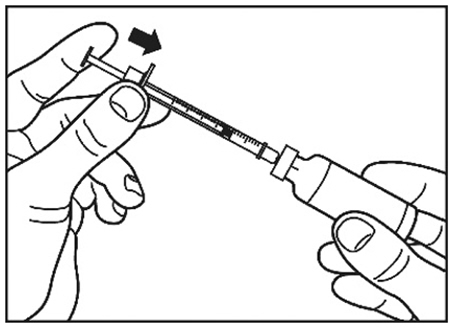
Draw air into the syringe equal to your insulin dose (see Figure C ). Put the needle through the rubber top of the vial and push the plunger to inject the air into the vial (see Figure D ).
|
|
| ( Figure C ) | ( Figure D ) |

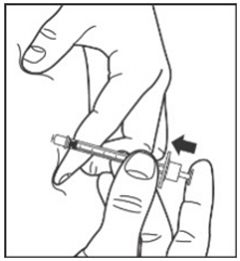
Step 4:
Leave the syringe in the vial and turn both upside down. Hold the syringe and vial firmly in one hand. Make sure the tip of the needle is in the insulin. With your free hand, pull the plunger to withdraw the correct dose into the syringe (see Figure E ).
 ( Figure E )
( Figure E )
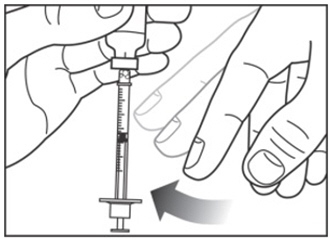
Step 5:
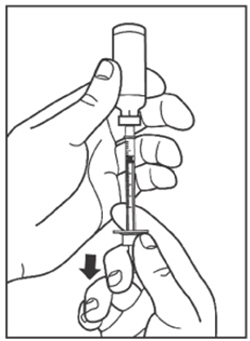
Before you take the needle out of the vial, check the syringe for air bubbles. If bubbles are in the syringe, hold the syringe straight up and tap the side of the syringe until the bubbles float to the top. Push the bubbles out with the plunger and draw insulin back in until you have the correct dose (see Figure F ).
 ( Figure F )
( Figure F )
Step 6:
Remove the needle from the vial. Do not let the needle touch anything. You are now ready to inject.
Giving your MERILOG injection with a syringe
- Inject your insulin exactly as your healthcare provider has shown you.
- MERILOG starts acting fast. You should eat a meal within 5 to 10 minutes after you take your dose of MERILOG.
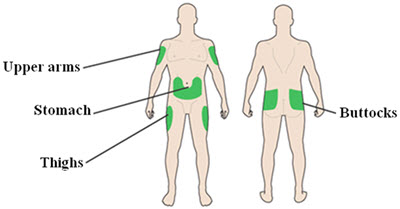
Step 7:
- Choose your injection site: MERILOG is injected under the skin (subcutaneously) of your stomach area (abdomen), buttocks, upper legs (thighs) or upper arms (see Figure G ).
- Do not use the exact same spot for each injection. Change (rotate) your injection sites within the area you choose for each dose to reduce your risk of getting pits in the skin or thickened skin (lipodystrophy) and skin with lumps (localized cutaneous amyloidosis) at the injection sites.
- Do not inject where the skin has pits, is thickened, or has lumps.
- Do not inject where the skin is tender, bruised, scaly or hard, or into scars or damaged skin.
 ( Figure G )
( Figure G ) - Wipe the skin with an alcohol swab to clean the injection site. Let the injection site dry before you inject your dose (see Figure H ).
 ( Figure H )
( Figure H )
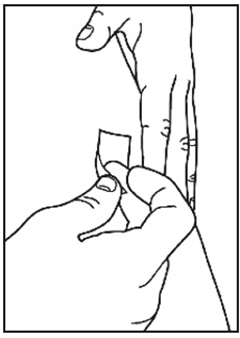
Step 8:
- Pinch the skin.
- Insert the needle in the way your healthcare provider showed you.
- Release the skin.
- Slowly push in the plunger of the syringe all the way, making sure you have injected all the insulin.
- Leave the needle in the skin for about 10 seconds (see Figure I ).
 ( Figure I )
( Figure I )
Step 9:
- Pull the needle straight out of your skin.
- Gently press the injection site for several seconds. Do not rub the area.
- Do not recap the used needle. Recapping the needle can lead to a needle-stick injury.
Disposing of used needles and syringes
- Put your used needles and syringes in a FDA-cleared sharps disposal container right away after use. Do not throw away (dispose of) loose needles and syringes in your household trash.
- If you do not have a FDA-cleared sharps container, you may use a household container that is:
- made of a heavy-duty plastic,
- can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out,
- upright and stable during use,
- leak resistant, and
- properly labeled to warn of hazardous waste inside the container.
- When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to dispose of your sharps disposal container. There may be state or local laws about how you should throw away used needles and syringes. For more information about safe sharps disposal, and for specific information about sharps disposal in the state that you live in, go to the FDA's website at: http://www.fda.gov/safesharpsdisposal.
- Do not dispose of your used sharps disposal container in your household trash unless your community guidelines permit this. Do not recycle your used sharps disposal container.
How should I store MERILOG?
Unopened (not in-use) MERILOG vials
- Store unused MERILOG vials in the refrigerator between 36°F to 46°F (2°C to 8°C).
- Do not freeze MERILOG.
- Keep MERILOG away from direct heat and light.
- If a vial has been frozen or overheated, throw it away.
- Unopened vials can be used until the expiration date on the carton and label if they have been stored in the refrigerator.
- Unopened vials should be thrown away after 28 days if they are stored at room temperature.
After MERILOG vials have been opened (in-use)
- Store in-use (opened) MERILOG vials in a refrigerator between 36°F to 46°F (2°C to 8°C) or at room temperature below 86°F (30°C) for up to 28 days .
- Do not freeze MERILOG.
- Do not expose MERILOG to excessive heat or light.
- If a vial has been frozen, throw it away.
- The MERILOG vial you are using should be thrown away after 28 days, even if it still has insulin left in it.
Manufactured by: sanofi-aventis U.S. LLC Morristown, NJ 07960 A SANOFI COMPANY U.S. License No. 1752
©2025 Sanofi. All rights reserved. All trademarks mentioned in this document are the property of the Sanofi group.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Approved: May 2025
Mechanism of Action
The primary activity of insulin, including insulin aspart products is the regulation of glucose metabolism. Insulin and its analogs lower blood glucose by stimulating peripheral glucose uptake, especially by skeletal muscle and fat, and by inhibiting hepatic glucose production. Insulin inhibits lipolysis and proteolysis, and enhances protein synthesis.