Get your patient on Opvee - Nalmefene Hydrochloride spray (Nalmefene Hydrochloride)
Opvee - Nalmefene Hydrochloride spray prescribing information
INDICATIONS AND USAGE
OPVEE nasal spray is indicated for the emergency treatment of known or suspected overdose induced by natural or synthetic opioids in adults and pediatric patients aged 12 years and older, as manifested by respiratory and/or central nervous system depression.
OPVEE nasal spray is intended for immediate administration as emergency therapy in settings where opioids may be present.
OPVEE nasal spray is not a substitute for emergency medical care.
DOSAGE AND ADMINISTRATION
- OPVEE nasal spray is for intranasal use only (2.1 )
- Seek emergency care immediately after use (2.1 )
- Administer a single spray of OPVEE nasal spray intranasally into nose. (2.2 )
- Administer additional doses of OPVEE nasal spray, using a new nasal spray with each dose, if the patient does not respond or responds and then relapses into respiratory depression, additional doses of OPVEE nasal spray may be given every 2 to 5 minutes until emergency medical assistance arrives. (2.2 )
- Additional supportive and/or resuscitative measures may be helpful while awaiting emergency medical assistance. (2.2 )
Important Administration Instructions
- OPVEE is for intranasal use only.
- The device is ready to use. No device assembly is required.
- Do not prime or test prior to administration. OPVEE nasal spray delivers its entire contents automatically, upon activation.
- Do not attempt to reuse OPVEE. Each unit-dose device contains a single dose of nalmefene and cannot be reused.
- No device assembly is required.
- Because treatment of suspected opioid overdose must be performed by someone other than the patient, instruct the prescription recipient to inform those around them about the presence of OPVEE nasal spray and the Instructions for Use .
- Instruct the patient or caregiver to read the Instructions for Use at the time they receive a prescription for OPVEE nasal spray. Emphasize the following instructions to the patient or caregiver:
- Administer OPVEE nasal spray as quickly as possible because prolonged respiratory depression may result in damage to the central nervous system or death.
- Always seek emergency medical assistance after administration of the first dose of OPVEE nasal spray in the event of a suspected, potentially life-threatening opioid emergency. Keep the patient under continued surveillance until emergency personnel arrive.
- Additional doses of OPVEE nasal spray may be required until emergency medical assistance becomes available.
- Re-administer OPVEE nasal spray, using a new nasal spray, in the nose, every 2 to 5 minutes if the patient does not respond or responds and then relapses into respiratory depression.
- Administer OPVEE nasal spray according to the printed instructions on the Quick Start Guide and the Instructions for Use .
- Place the patient in the supine position. Prior to administration, be sure the device nozzle is inserted in the nose of the patient and provide support to the back of the neck to allow the head to tilt back. Do not prime or test the device prior to administration.
- To administer the dose, press firmly on the device plunger and remove the device nozzle from the nose after use.
- If the patient responds by waking up to the voice or touch or starts breathing normally, place the patient on their side (recovery position) as shown in the Instructions for Use and call for emergency medical assistance immediately after administration of the first dose of OPVEE nasal spray.
Dosing in Adults and Pediatric Patients aged 12 years and older
Initial Dosing:
The recommended initial dose of OPVEE nasal spray in adults and pediatric patients aged 12 years and older is one spray delivered by intranasal administration, which delivers 2.7 mg of nalmefene.
Repeat Dosing:
Seek emergency medical assistance as soon as possible after intranasal administration of the first dose of OPVEE nasal spray. The requirement for repeat doses of OPVEE nasal spray (2.7 mg) depends upon the amount, type, and route of administration of the opioid being antagonized.
If the patient responds to OPVEE nasal spray and relapses back into respiratory depression before emergency assistance arrives, administer an additional dose of OPVEE in the opposite nostril using a new OPVEE nasal spray and continue surveillance of the patient.
If the desired response is not obtained after 2 to 5 minutes, administer an additional dose of OPVEE using a new OPVEE nasal spray device. If there is still no response and additional doses are available, administer additional doses of OPVEE nasal spray every 2 to 5 minutes using a new OPVEE nasal spray device with each dose until emergency medical assistance arrives.
Additional supportive and/or resuscitative measures may be helpful while awaiting emergency medical assistance.
Dosing Modifications due to Partial Agonists or Mixed Agonists/Antagonists
Reversal of respiratory depression by partial agonists or mixed agonist/antagonists, such as buprenorphine and pentazocine, may be incomplete and require repeated administration of OPVEE nasal spray using a new nasal spray device [see Warnings and Precautions (5.2) ] .
DOSAGE FORMS AND STRENGTHS
Nasal spray: 2.7 mg nalmefene per device. Each unit-dose nasal spray device delivers a single spray containing 2.7 mg of nalmefene.
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
Life-sustaining therapy for opioid overdose should not be withheld (see Clinical Considerations ). There are no available data on nalmefene use in pregnant women to evaluate for a drug-associated risk of major birth defects or miscarriage. In animal reproduction studies, no embryotoxic effects on embryo-fetal development were observed in rats and rabbits treated with nalmefene at exposures at least 6 times (rats) and up to 20 times (rabbits) the exposure at two human nasal doses of 5.4 mg (see Data ) .
The background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-associated maternal and/or embryo/fetal risk
An opioid overdose is a medical emergency and can be fatal for the pregnant woman and fetus if left untreated. Treatment with OPVEE for opioid overdose should not be withheld because of potential concerns regarding the effects of OPVEE on the fetus.
Data
Animal Data
Reproduction studies have been performed in rats (up to 1200 mg/m 2 /day) and rabbits (up to 2400 mg/m 2 /day) by oral administration of nalmefene and in rabbits by intravenous administration up to 96 mg/m 2 /day. No effects on embryo-fetal development were observed at exposures at least 6 times (rats) and up to 20 times (rabbits) the exposure corresponding to a human dose of 5.4 mg (two nalmefene nasal sprays) on an AUC basis. The treatment in rats did not affect offspring survival.
Lactation
Risk Summary
There are no data on the presence of nalmefene and its metabolites in human milk, the effects of nalmefene on the breastfed child, or the effects on milk production. Nalmefene and its metabolites are present in rat milk (see Data ). When a drug is present in animal milk, it is likely that the drug will be present in human milk.
Data
Nalmefene and its metabolites were secreted into rat milk, reaching concentrations approximately three times those in plasma at one hour and decreasing to about half the corresponding plasma concentrations by 24 hours following bolus administration. The concentration of nalmefene in animal milk does not necessarily predict the concentration of drug in human milk.
Pediatric Use
The safety and effectiveness of OPVEE nasal spray for the emergency treatment of known or suspected opioid overdose in adults and pediatric patients aged 12 years and older, as manifested by respiratory and/or central nervous system depression, have been established.
Use for this indication in this age group is supported by adult studies and pharmacokinetic simulation [see Clinical Pharmacology (12.3) ] . There have been no studies conducted to evaluate the use of OPVEE nasal spray in pediatric patients.
The safety and effectiveness of OPVEE nasal spray for the emergency treatment of known or suspected opioid overdose, as manifested by respiratory and/or central nervous system depression have not been established in pediatric patients younger than 12 years of age.
Geriatric Use
Clinical studies of OPVEE nasal spray did not include subjects aged 65 and over. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. Geriatric patients have a greater frequency of decreased hepatic, renal, or cardiac function and of concomitant disease or other drug therapy. Therefore, the systemic exposure of nalmefene can be higher in these patients.
Hepatic Impairment
Hepatic impairment substantially reduces the clearance of nalmefene [see Clinical Pharmacology (12.3) ]. For single episodes of opioid antagonism, adjustment of OPVEE nasal spray dosage is not required.
Renal Impairment
Renal impairment substantially reduces the clearance of nalmefene [see Clinical Pharmacology (12.3) ]. For single episodes of opioid antagonisms, adjustment of OPVEE nasal spray dosage is not required.
CONTRAINDICATIONS
OPVEE nasal spray is contraindicated in patients known to be hypersensitive to nalmefene or to any of the other ingredients.
WARNINGS AND PRECAUTIONS
- Risk of Recurrent Respiratory and Central Nervous System Depression : While the duration of action of nalmefene is as long as most opioids, a recurrence of respiratory depression is possible, therefore, keep patient under continued surveillance and administer repeat doses of OPVEE using a new nasal spray with each dose, as necessary, while awaiting emergency medical assistance (5.1 )
- Limited Efficacy with Partial Agonists or Mixed Agonist/Antagonists : Reversal of respiratory depression caused by partial agonists or mixed agonists/antagonists, such as buprenorphine and pentazocine, may be incomplete. Larger or repeat doses may be required. (5.2 )
- Precipitation of Severe Opioid Withdrawal : Use in patients who are opioid dependent may precipitate opioid withdrawal. In neonates, opioid withdrawal may be life-threatening if not recognized and properly treated. Monitor for the development of opioid withdrawal. (5.3 )
- Risk of Cardiovascular (CV) Effects : Abrupt postoperative reversal of opioid depression may result in adverse CV effects. These events have primarily occurred in patients who had preexisting CV disorders or received other drugs that may have similar adverse CV effects. Monitor these patients closely in an appropriate healthcare setting after use of nalmefene hydrochloride. (5.3 )
- Risk of Opioid Overdose from Attempts to Overcome the Blockade : Attempts to overcome opioid withdrawal symptoms caused by opioid antagonists with high or repeated doses of exogenous opioids may lead to opioid intoxication and death (5.4 )
Risk of Recurrent Respiratory and Central Nervous System Depression
Respiratory depression in the community overdose setting may be complex and involve the effects of multiple or unknown drugs, some of which may be long-acting opioids. While the duration of action of nalmefene is as long as most opioids, a recurrence of respiratory depression is possible, even after an apparently adequate initial response to OPVEE nasal spray treatment [See Clinical Pharmacology, Pharmacodynamics (12.3) ] . Therefore, it is necessary to seek emergency medical assistance immediately after administration of the first dose of OPVEE nasal spray and to keep the patient under continued surveillance. A second dose may be necessary if there is recurrence of symptoms of opioid overdose. Additional supportive and/or resuscitative measures may be helpful while awaiting emergency medical assistance [see Dosage and Administration (2.2) ].
Risk of Limited Efficacy with Partial Agonists or Mixed Agonist/Antagonists
Reversal of respiratory depression by partial agonists or mixed agonist/antagonists such as buprenorphine and pentazocine, may be incomplete. Repeat doses of OPVEE nasal spray may be required to antagonize buprenorphine because the latter has a long duration of action due to its slow rate of binding and subsequent slow dissociation from the opioid receptor [see Dosage and Administration (2.3) ] . Buprenorphine antagonism is characterized by a gradual onset of the reversal effects and a decreased duration of action of the normally prolonged respiratory depression.
Precipitation of Severe Opioid Withdrawal
The use of OPVEE in patients who are opioid dependent may precipitate opioid withdrawal characterized by the following signs and symptoms: body aches, diarrhea, tachycardia, fever, runny nose, sneezing, piloerection, sweating, yawning, nausea or vomiting, nervousness, restlessness or irritability, shivering or trembling, abdominal cramps, weakness, and increased blood pressure.
Abrupt postoperative reversal of opioid depression after using OPVEE may result in nausea, vomiting, sweating, tremulousness, tachycardia, hypotension, hypertension, seizures, ventricular tachycardia and fibrillation, pulmonary edema, and cardiac arrest. Death, coma, and encephalopathy have been reported as sequelae of these events. These events have primarily occurred in patients who had pre-existing cardiovascular disorders or received other drugs that may have similar adverse cardiovascular effects. After use of OPVEE, monitor patients with pre-existing cardiac disease or patients who have received medications with potential adverse cardiovascular effects for hypotension, ventricular tachycardia or fibrillation, and pulmonary edema in an appropriate healthcare setting. It has been suggested that the pathogenesis of pulmonary edema associated with the use of nalmefene is similar to neurogenic pulmonary edema, i.e., a centrally mediated massive catecholamine response leading to a dramatic shift of blood volume into the pulmonary vascular bed resulting in increased hydrostatic pressures.
OPVEE is not indicated for use in patients less than 12 years of age. In neonates, opioid withdrawal may be life-threatening if not recognized and properly treated and may include the following signs and symptoms: convulsions, excessive crying, and hyperactive reflexes. Monitor the patient for the development of the signs and symptoms of opioid withdrawal. There may be clinical settings, particularly the postpartum period in neonates with known or suspected exposure to maternal opioid use, where it is preferable to avoid the abrupt precipitation of opioid withdrawal symptoms. In these settings, use an alternative, opioid antagonist product that can be titrated to effect and, where applicable, dosed according to weight. [see Use in Specific Populations (8.4) ] .
Risk of Opioid Overdose from Attempts to Overcome the Blockade
OPVEE is unlikely to produce acute withdrawal symptoms in non-opioid dependent patients. The use of OPVEE nasal spray in patients who are opioid dependent may precipitate opioid withdrawal. Attempting to overcome opioid withdrawal symptoms caused by opioid antagonists with high or repeated doses of exogenous opioids could lead to opioid intoxication and death. Inform patients of the potential consequences of trying to overcome the opioid blockade. Get emergency medical assistance as soon as possible after use of OPVEE nasal spray regardless of withdrawal symptoms.
ADVERSE REACTIONS
The following serious adverse reactions are discussed elsewhere in the labeling:
- Recurrent Respiratory and Central Nervous System Depression [see Warnings and Precautions (5.1) ]
- Precipitation of Severe Opioid Withdrawal [see Warnings and Precautions (5.3) ]
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to the rates in clinical trials of another drug and may not reflect the rates observed in practice.
The safety of OPVEE nasal spray is supported by safety and pharmacokinetic studies of OPVEE nasal spray in healthy subjects in a normal state and under steady state opioid agonism. The following adverse reactions were observed.
In a pharmacokinetic study of 66 healthy adult volunteers exposed to one spray of OPVEE nasal spray in one nostril the most common adverse reactions were: nasal discomfort and dizziness.
In a second pharmacokinetic study of 24 healthy adult volunteers exposed to one spray of OPVEE nasal spray in one nostril, two sprays of OPVEE nasal spray in one nostril or one spray of OPVEE nasal spray in each nostril, the most common adverse reactions were: rhinalgia, nasal congestion, nasal discomfort and nausea.
In a pharmacodynamic study of 61 healthy adult volunteers exposed to one spray of OPVEE nasal spray in one nostril, the most common adverse reactions were: headache, nausea, hot flush and dizziness.
| Nalmefene 2.7 mg | Nalmefene 5.4 mg | ||||
|---|---|---|---|---|---|
| System Organ Class Preferred Term | Total 2.7 mg N=150 n (%) | PD Study N=61 n (%) | PK Studies N=89 n (%) | PK Study (1 spray in each nostril) N=23 n (%) | PK Study (2 sprays in one nostril) N=24 n (%) |
| PK Studies OPNT003-PK-001 + OPNT003-PK-002 and PD Study OPNT003-OOD-001 | |||||
| Respiratory, thoracic and mediastinal disorders | |||||
| Nasal discomfort | 43 (28.7%) | 5 (8.2%) | 38 (42.7%) | 3 (13.0%) | 3 (12.5%) |
| Nasal congestion | 6 (4.0%) | 2 (3.3%) | 4 (4.5%) | 1 (4.3%) | 4 (16.7%) |
| Throat irritation | 6 (4.0%) | 3 (4.9%) | 3 (3.4%) | 0 | 0 |
| Rhinalgia | 4 (2.7%) | 1 (1.6%) | 3 (3.4%) | 2 (8.7%) | 6 (25.0%) |
| Dyspnea | 2 (1.3%) | 2 (3.3%) | 0 | 0 | 0 |
| Oropharyngeal pain | 2 (1.3%) | 2 (3.3%) | 0 | 1 (4.3%) | 1 (4.2%) |
| Nervous system disorders | |||||
| Headache | 40 (26.7%) | 34 (55.7%) | 6 (6.7%) | 1 (4.3%) | 0 |
| Dizziness | 14 (9.3%) | 9 (14.8%) | 5 (5.6%) | 0 | 1 (4.2%) |
| Dysgeusia | 3 (2.0%) | 2 (3.3%) | 1 (1.1%) | 0 | 0 |
| Paresthesia | 2 (1.3%) | 2 (3.3%) | 0 | 1 (4.3%) | 1 (4.2%) |
| Presyncope | 0 | 0 | 0 | 1 (4.3%) | 0 |
| Gastrointestinal disorders | |||||
| Nausea | 25 (16.7%) | 22 (36.1%) | 3 (3.4%) | 5 (21.7%) | 1 (4.2%) |
| Vomiting | 9 (6.0%) | 7 (11.5%) | 2 (2.2%) | 1 (4.3%) | 0 |
| Abdominal pain | 2 (1.3%) | 1 (1.6%) | 1 (1.1%) | 0 | 0 |
| Dry mouth | 1 (0.7%) | 1 (1.6%) | 0 | 1 (4.3%) | 0 |
| Constipation | 0 | 0 | 0 | 0 | 1 (4.2%) |
| Vascular disorders | |||||
| Hot flush | 12 (8.0%) | 12 (19.7%) | 0 | 0 | 0 |
| Psychiatric disorders | |||||
| Anxiety | 7 (4.7%) | 7 (11.5%) | 0 | 0 | 0 |
| Agitation | 2 (1.3%) | 2 (3.3%) | 0 | 0 | 0 |
| Claustrophobia | 2 (1.3%) | 2 (3.3%) | 0 | 0 | 0 |
| Insomnia | 1 (0.7%) | 0 | 1 (1.1%) | 1 (4.3%) | 0 |
| General disorders and administration site conditions | |||||
| Fatigue | 6 (4.0%) | 3 (4.9%) | 3 (3.4%) | 0 | 0 |
| Chills | 2 (1.3%) | 2 (3.3%) | 0 | 0 | 0 |
| Chest discomfort | 0 | 0 | 0 | 1 (4.3%) | 0 |
| Skin and subcutaneous tissue disorders | |||||
| Erythema | 3 (2.0%) | 0 | 3 (3.4%) | 1 (4.3%) | 1 (4.2%) |
| Hyperhidrosis | 3 (2.0%) | 3 (6.6%) | 0 | 0 | 1 (4.2%) |
| Urticaria | 0 | 0 | 0 | 0 | 1 (4.2%) |
| Metabolism and nutrition disorders | |||||
| Decreased appetite | 3 (2.0%) | 2 (3.3%) | 1 (1.1%) | 0 | 0 |
| Infections and infestations | |||||
| Rhinitis | 1 (0.7%) | 0 | 1 (1.1%) | 1 (4.3%) | 0 |
| Eye disorders | |||||
| Dry eye | 0 | 0 | 0 | 1 (4.3%) | 0 |
| Cardiac disorders | |||||
| Tachycardia | 0 | 0 | 0 | 1 (4.3%) | 0 |
Adverse reaction information was obtained following administration of nalmefene injection to 152 normal volunteers and in controlled clinical trials to 1127 patients for the treatment of opioid overdose or for postoperative opioid reversal.
| Adverse Reaction | Nalmefene | Placebo |
|---|---|---|
| N=1127 | N=77 | |
| Nausea | 18% | 6% |
| Vomiting | 9% | 4% |
| Tachycardia | 5% | - |
| Hypertension | 5% | - |
| Postoperative Pain | 4% | N/A |
| Fever | 3% | - |
| Dizziness | 3% | 1% |
| Headache | 1% | 4% |
| Chills | 1% | - |
| Hypotension | 1% | - |
| Vasodilatation | 1% | - |
Incidence less than 1%
Cardiovascular : Bradycardia, arrhythmia Digestive : Diarrhea, dry mouth Nervous System : Somnolence, depression, agitation, nervousness, tremor, confusion, withdrawal syndrome, myoclonus Respiratory : Pharyngitis Skin : Pruritus Urogenital : Urinary retention
The incidence of adverse events was highest in patients who received more than the recommended dose of nalmefene injection.
Postmarketing Experience
The following adverse reactions have been identified during post-approval use of nalmefene. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Abrupt reversal of opioid depression using nalmefene in both postoperative and emergency department settings has resulted in nausea, vomiting, sweating, tremulousness, seizures, and cardiovascular instability including tachycardia, hypotension, hypertension, ventricular tachycardia and fibrillation, pulmonary edema, and cardiac arrest. Death, coma, and encephalopathy have been reported as sequelae of these events. These events have primarily occurred in patients who had pre-existing cardiovascular disorders or received other drugs that may have similar adverse cardiovascular effects.
In persons who were physically dependent on opioids, abrupt reversal of opioid effects has precipitated an acute withdrawal syndrome. Signs and symptoms have included: body aches, fever, sweating, runny nose, sneezing, piloerection, yawning, weakness, shiver or trembling, nervousness, restlessness or irritability, diarrhea, nausea or vomiting, abdominal cramps, increased blood pressure, tachycardia. In some patients, there may be aggressive behavior upon abrupt reversal of an opioid overdose. In the neonate, opioid withdrawal symptoms also included convulsions, excessive crying, and hyperactive reflexes.
DESCRIPTION
OPVEE (nalmefene) nasal spray is a pre-filled, unit-dose intranasal spray.
Nalmefene, an opioid antagonist, is a 6-methylene analogue of naltrexone. The molecular structure of nalmefene is presented below:
Molecular Formula: C 21 H 25 NO 3 ∙HCl
Molecular Weight: 375.9, CAS # 58895-64-0
Chemical Name: 17-(Cyclopropylmethyl)-4,5α-epoxy-6-methylenemorphinan-3,14-diol, hydrochloride salt.
Nalmefene is a white to off-white crystalline powder which is freely soluble in methanol and water, with a pK of 7.63.
Each OPVEE nasal spray unit delivers 2.7 mg nalmefene (equivalent to 3mg nalmefene hydrochloride) in 0.1 mL solution.
Inactive ingredients include benzalkonium chloride, disodium ethylenediaminetetraacetate, dodecylmaltoside, sodium chloride, and purified water. The pH range is 4.1 to 4.9.
CLINICAL PHARMACOLOGY
Mechanism of Action
OPVEE is an antagonist at opioid receptors.
Pharmacodynamics
Nalmefene reverses the effects of natural and synthetic opioids, including respiratory depression, sedation, and hypotension. Pharmacodynamic studies have shown that nalmefene injection has a longer duration of action than naloxone injection at fully reversing doses. Nalmefene has no opioid agonist activity.
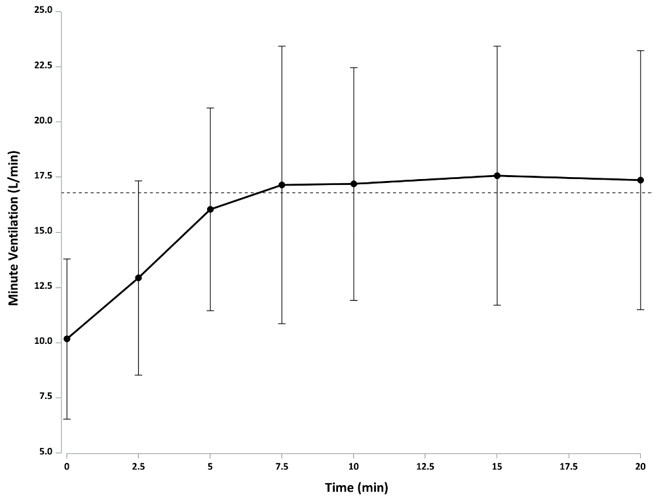
The effect of 2.7 mg OPVEE on remifentanil-induced respiratory depression in an experimental ventilatory-response to hypercapnia model, assessed by changes in minute ventilation (MV), was evaluated in sixty-one opioid-experienced, non-dependent subjects. In this study subjects started receiving a hypercapnic gas mixture (50% O2, 43% N2, 7% CO2) at -25 minutes. Just prior to initiation of remifentanil infusion at -15 minutes is the baseline MV (marked as 100% in Figure 1 and marked as observed data as liters/minute in Figure 2). Fifteen minutes after initiating remifentanil infusion, nadir in minute ventilation is observed at time zero, at which point OPVEE was administered. The subjects were then monitored for changes in MV over 120 minutes. Following OPVEE administration the time to onset of effect, that is onset of reversal of respiratory depression, was observed between 2.5 to 5 minutes (Figure 1 and Figure 2). At 5 minutes the estimated mean increase in minute ventilation was 5.745 L/min (Figure 2). Full recovery of respiratory drive was noted between 5 and 15 minutes after OPVEE administration (Figure 1 and Figure 2).
Figure 1 : Percentage recovery of respiratory drive after infusion of remifentanil in CO2 stimulated minute ventilation (mean +/- standard deviation) in adult healthy volunteers treated with OPVEE (nalmefene) nasal spray
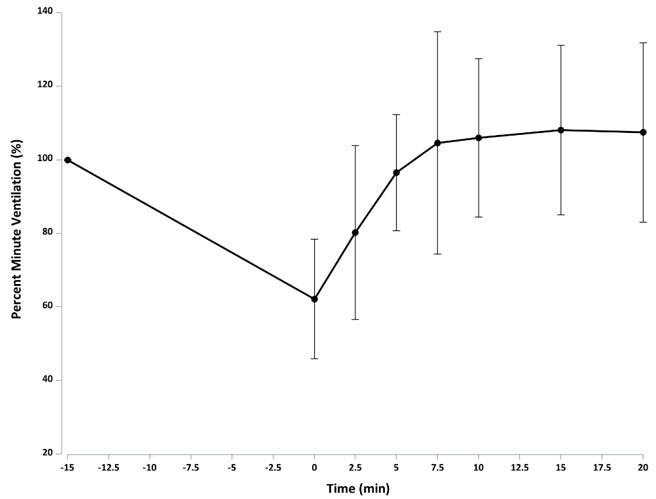
Figure 2: Reversal of Remifentanil-Induced Respiratory Depression (Mean Minute Ventilation +/- Standard Deviation) by OPVEE (nalmefene) nasal spray
| Remifentanil (an initial bolus of 0.5 µg/kg dose followed by an infusion rate of 0.175 µg/kg/min) was administered for 15 min prior to test agents and continued for the duration of the study. The dashed line represents the mean minute ventilation (MV) prior to remifentanil administration. |
|
Based on population pharmacokinetic/pharmacodynamic model simulations, the EC50 (drug concentration at which pharmacological effect is half maximum change in response) was 1.50 ng/mL for OPVEE following a single 2.7 mg administration. The time to reach EC50 was 4 minutes for OPVEE. The plasma concentrations remained above the EC50 for 5.94 hours for OPVEE.
Nalmefene is not known to produce respiratory depression, psychotomimetic effects, or pupillary constriction. No pharmacological activity was observed when nalmefene was administered in the absence of opioid agonists.
Nalmefene has not been shown to produce tolerance, physical dependence, or abuse potential.
Nalmefene can produce acute withdrawal symptoms in individuals who are opioid dependent.
Pharmacokinetics
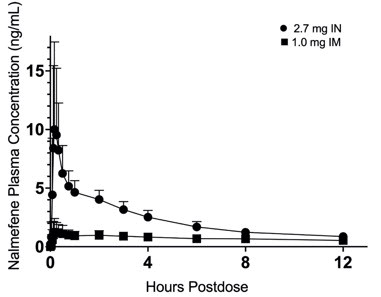
In a pharmacokinetic study (OPNT003-PK-001) in 68 healthy adult subjects, the relative bioavailability of one 2.7 mg OPVEE nasal spray in one nostril (0.1 mL of 27 mg/mL nalmefene), was compared to a single dose of nalmefene 1.0 mg administered as an intramuscular injection. Subjects remained fully supine and were instructed to hold their breath during the intranasal spray administration. The pharmacokinetic parameters obtained in this study are shown in Table 3 and the plasma concentration time profiles of nalmefene are presented in Figure 3.
| Parameter | OPVEE | Nalmefene IM |
|---|---|---|
| NA Not applicable | ||
| T max (h) T max presented as median (range) | 0.250 (0.0833-2.00) | 0.33 (0.117-18.0) |
| C max (ng/mL) Arithmetic mean | 10.4 (62.6) | 1.50 (59.4) |
| AUC 0-2.5min (ng-hr/mL) | 0.00763 (233) | 0.00168 (186) |
| AUC 0-5min (ng-hr/mL) | 0.0599 (201) | 0.0102 (142) |
| AUC 0-10min (ng-hr/mL) | 0.523 (124) | 0.0639 (118) |
| AUC 0-15min (ng-hr/mL) | 1.20 (94.2) | 0.142 (98.6) |
| AUC 0-20min (ng-hr/mL) | 1.89 (77.2) | 0.228 (84.5) |
| AUC 0-30min (ng-hr/mL) | 3.07 (60.4) | 0.405 (69.2) |
| AUC 0-inf (ng-hr/mL) | 40.6 (22.0) | 16.8 (18.7) |
| F rel | 0.806 (10.9) | NA |
| T ½ (h) | 11.4 (20.8) | 10.6 (18.5) |
| Values represent the mean and standard deviation (n=68) |
| Figure 3: Mean Plasma Concentration-Time Profiles of Nalmefene (a) 0-12 hours and (b) 0-60 minutes Following Intranasal (IN) Administration of OPVEE nasal spray (2.7 mg) and Intramuscular (IM) Injection of Nalmefene (1.0 mg) |
| (a) |
 |
| (b) |
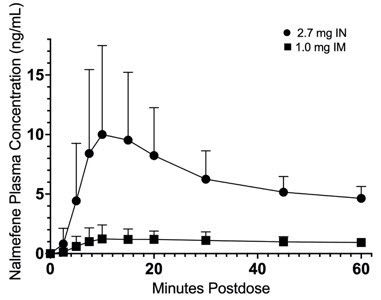 |
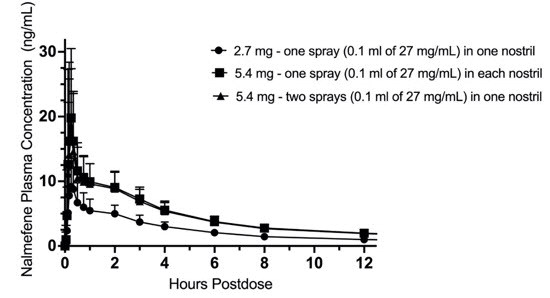
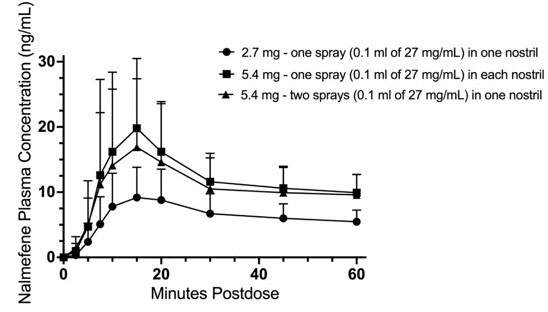
In a second pharmacokinetic study (OPNT003-PK-002) in 24 healthy adult subjects, one 2.7 mg OPVEE nasal spray in one nostril was compared with two 2.7 mg OPVEE nasal sprays in one nostril and one 2.7 mg OPVEE nasal spray in each nostril. Subjects remained fully supine and were instructed to hold their breath during the intranasal spray administration. The pharmacokinetic parameters obtained in this study are shown in Table 4 and the plasma concentration time profiles of nalmefene are presented in Figure 4.
| Parameter | OPVEE 2.7mg (one spray) | OPVEE 5.4mg (one spray in each nostril) | OPVEE 5.4mg (two sprays in one nostril) |
|---|---|---|---|
| T max (h) T max presented as median (range) | 0.267 (0.167-2.03) | 0.250 (0.117-3.00) | 0.250 (0.117-2.03) |
| C max (ng/mL) | 9.75 (49.4) | 18.9 (88.0) | 16.1 (62.9) |
| AUC 0-2.5min (ng-hr/mL) | 0.00594 (134) | 0.0163 (217) | 0.0172 (117) |
| AUC 0-5min (ng-hr/mL) | 0.0446 (99.6) | 0.110 (161) | 0.108 (92.9) |
| AUC 0-10min (ng-hr/mL) | 0.388 (72.1) | 0.828 (102) | 0.717 (93.2) |
| AUC 0-15min (ng-hr/mL) | 0.999 (65.9) | 2.08 (81.8) | 1.73 (83.0) |
| AUC 0-20min (ng-hr/mL) | 1.66 (61.3) | 3.42 (69.9) | 2.85(74.3) |
| AUC 0-30min (ng-hr/mL) | 2.83 (56.0) | 5.63 (57.7) | 4.78 (60.8) |
| AUC 0-inf (ng-hr/mL) | 45.8 (21.7) | 88.1 (18.3) | 83.8 (22.0) |
| T ½ (h) Arithmetic mean | 11.4 (22.0) | 11.3 (16.6) | 11.3 (16.5) |
| Values represent the mean and standard deviation (n=24) |
| Figure 4: Mean Plasma Concentration of Nalmefene, (a) 0-12 hours and (b) 0-60 minutes Following Intranasal (IN) Administration of 2.7 mg Nalmefene (One OPVEE nasal spray in One Nostril), IN Dose of 5.4 mg Nalmefene (One OPVEE nasal spray in Each Nostril) and IN Dose of 5.4 mg Nalmefene (Two OPVEE nasal sprays in One Nostril) |
| (a) |
|
| (b) |
|
Absorption
After administration of one 2.7 mg OPVEE nasal spray to healthy adult subjects, the median T max for OPVEE was 0.250 hours, compared to 0.33 hours for the intramuscular nalmefene.
After administration of two 2.7 mg OPVEE nasal sprays (total dose 5.4mg) to healthy adult subjects, the median T max for OPVEE was 0.250 hours.
The dose normalized area under the curve (AUC 0-inf ) to infinity is similar for one 2.7 mg OPVEE nasal spray in one nostril and one 2.7 mg OPVEE nasal spray in each nostril with a geometric mean ratio of 96.23% (90%CI 92.00%-100.65%). The dose normalized AUC 0-inf is also similar for one 2.7 mg OPVEE nasal spray in one nostril and two 2.7 mg OPVEE nasal sprays in one nostril with a geometric mean ratio of 91.19% (90%CI 87.19%-95.38%).
The mean bioavailability (F rel ) of OPVEE was 0.806 relative to intramuscular administration of nalmefene.
Distribution
Following a 1 mg parenteral dose, nalmefene was rapidly distributed. In a study of brain receptor occupancy, a 1 mg dose of nalmefene blocked over 80% of brain opioid receptors within 5 minutes after administration. The apparent volumes of distribution centrally (Vd) and at steady-state (Vss) are 3.9 ± 1.1 L/kg and 8.6 ± 1.7 L/kg, respectively. Ultrafiltration studies of nalmefene have demonstrated that 45% (CV 4.1%) is bound to plasma proteins over a concentration range of 0.1 to 2μg/mL. An in vitro determination of the distribution of nalmefene in human blood demonstrated that nalmefene distributed 67% (CV 8.7%) into red blood cells and 39% (CV 6.4%) into plasma. The whole blood to plasma ratio was 1.3 (CV 6.6%) over the nominal concentration range in whole blood from 0.376 to 30 ng/mL.
Elimination
After administration of 2.7 mg OPVEE nasal spray to healthy adult subjects, plasma concentrations have a terminal elimination half-life of 11.4 (%CV 20.8) hours. The apparent clearance of nalmefene is 75.7 (%CV 23.8) L/hr.
Specific Populations
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
The carcinogenic potential of nalmefene has not been evaluated.
Mutagenesis
Nalmefene did not have mutagenic activity in the Ames test with five bacterial strains or the mouse lymphoma assay. Clastogenic activity was not observed in the mouse micronucleus test or in the cytogenic bone marrow assay in rats. However, nalmefene did exhibit a weak but significant clastogenic activity in the human lymphocyte metaphase assay in the absence but not in the presence of exogenous metabolic activation.
Impairment of Fertility
Oral administration of nalmefene up to 1200 mg/m 2 /day did not affect fertility in rats at exposures at least 6 times the exposure corresponding to a human dose of 5.4 mg (two nalmefene nasal sprays) on an AUC basis.
HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
Each unit-dose nasal spray device delivers 2.7 mg of nalmefene (equivalent to 3 mg of nalmefene hydrochloride) in 0.1 mL. Each carton contains two unit-dose nasal spray devices.
NDC # 12496-0003-2
OPVEE is not made with natural rubber latex.
Storage and Handling
Store OPVEE nasal spray in the blister and cartons provided.
Store OPVEE nasal spray at controlled room temperature 15°C to 25°C (59°F to 77°F). Short-term excursions permitted between 4°C to 40°C (39°F to 104°F). Do not freeze. Protect from light.
Do not open individual blister packs or test nasal spray devices before use.
Each unit-dose nasal spray device sprays one (1) time and cannot be re-used.
INSTRUCTIONS FOR USE OPVEE (op vee) (nalmefene) nasal spray
The Instructions for Use contains information on how to give OPVEE nasal spray in response to a known or suspected opioid overdose in adults and children 12 years of age and older. You and your family members or caregivers should read the Instructions for Use that comes with OPVEE nasal spray before using it. Talk to your healthcare provider if you and your family members or caregivers have any questions about the use of OPVEE nasal spray.
 | Important Information You Need to Know Before Giving OPVEE nasal spray
| |
| Check for response Step 1. Shout "wake up" and shake the person gently. If there is no response, slow breathing, or no breathing, lay the person flat on their back ( Figure A ). |  Figure A Figure A | |
| Prepare to give OPVEE nasal spray Step 2 . Remove OPVEE nasal spray from the box. Peel off the back from the top corner to open the OPVEE nasal spray blister ( Figure B ). Step 3 . Hold the OPVEE nasal spray with your fingers on both sides of the nozzle and your thumb on the white plunger ( Figure C ). Do not press the plunger yet. |  Figure B Figure B 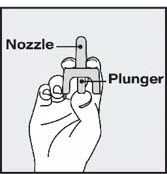 Figure C Figure C | |
| Give OPVEE nasal spray Step 4. Provide support behind the neck with your hand and tilt the person's head back ( Figure D ). Step 5. Gently insert the nozzle into one nostril until your fingers on either side of the nozzle are against the bottom of the person's nose. (Figure D ). Step 6. Press the plunger firmly to give the dose of OPVEE nasal spray in the nose. The dose has been delivered when the white plunger has been pushed all the way down until it stops. Step 7. Remove the OPVEE nasal spray from the nostril after the dose has been given. |  Figure D Figure D | |
After giving OPVEE nasal spray Step 8 . Call 911 or get emergency medical help right away ( Figure E ). Step 9. Move the person on their side (recovery position) ( Figure F ):
|  Figure E Figure E  Figure F Figure F  Figure G Figure G | |
Storing OPVEE nasal spray
| ||
For more information about OPVEE nasal spray, go to www.OPVEE.com or call 1-877-782-6966.
OPVEE ® is a registered trademark of Indivior Inc. ©2023 Indivior Inc. All Rights Reserved. Manufactured for: Indivior Inc., North Chesterfield, VA, 23235, USA
This Instructions for Use has been approved by the U.S. Food and Drug Administration. Issued: 06/2023
Mechanism of Action
OPVEE is an antagonist at opioid receptors.