Get your patient on Padcev (Enfortumab Vedotin)
Padcev patient education
Patient toolkit
Dosage & administration
Coverage
See specific coverage requirements, including prior authorization and step therapies.

Padcev prescribing information
WARNING: SERIOUS SKIN REACTIONS
- PADCEV can cause severe and fatal cutaneous adverse reactions including Stevens-Johnson syndrome (SJS) and Toxic Epidermal Necrolysis (TEN), which occurred predominantly during the first cycle of treatment, but may occur later.
- Closely monitor patients for skin reactions.
- Immediately withhold PADCEV and consider referral for specialized care for suspected SJS or TEN or severe skin reactions.
- Permanently discontinue PADCEV in patients with confirmed SJS or TEN; or Grade 4 or recurrent Grade 3 skin reactions [see Dosage and Administration (2.2 ), Warnings and Precautions (5.1 ), and Adverse Reactions (6.1 )].
INDICATIONS AND USAGE
PADCEV ® , in combination with pembrolizumab or pembrolizumab and berahyaluronidase alfa-pmph, as neoadjuvant treatment and then continued after cystectomy as adjuvant treatment, is indicated for the treatment of adult patients with muscle invasive bladder cancer (MIBC) who are ineligible for cisplatin-containing chemotherapy.
PADCEV ® , in combination with pembrolizumab or pembrolizumab and berahyaluronidase alfa-pmph, is indicated for the treatment of adult patients with locally advanced or metastatic urothelial cancer (mUC).
PADCEV, as a single agent, is indicated for the treatment of adult patients with locally advanced or mUC who:
- have previously received a programmed death receptor-1 (PD-1) or programmed death-ligand 1 (PD-L1) inhibitor and platinum-containing chemotherapy, or
- are ineligible for cisplatin-containing chemotherapy and have previously received one or more prior lines of therapy.
DOSAGE AND ADMINISTRATION
- For intravenous infusion only. Do not administer PADCEV as an intravenous push or bolus. Do not mix with, or administer as an infusion with, other medicinal products. (2.3 )
- MIBC: The recommended dose of PADCEV in combination with pembrolizumab or pembrolizumab and berahyaluronidase alfa-pmph is 1.25 mg/kg (up to a maximum dose of 125 mg) given as an intravenous infusion over 30 minutes. PADCEV is administered as neoadjuvant treatment on Days 1 and 8 of each 21-day cycle for 3 cycles or until disease progression that precludes curative intent cystectomy or unacceptable toxicity, followed by adjuvant treatment on Days 1 and 8 of each 21-day cycle for 6 cycles or until disease recurrence or unacceptable toxicity. (2.1 )
- Locally Advanced or mUC: The recommended dose of PADCEV in combination with pembrolizumab or pembrolizumab and berahyaluronidase alfa-pmph is 1.25 mg/kg (up to a maximum dose of 125 mg) given as an intravenous infusion over 30 minutes on Days 1 and 8 of a 21-day cycle until disease progression or unacceptable toxicity. (2.1 )
- The recommended dose of PADCEV as a single agent is 1.25 mg/kg (up to a maximum dose of 125 mg) given as an intravenous infusion over 30 minutes on Days 1, 8, and 15 of a 28-day cycle until disease progression or unacceptable toxicity. (2.1 )
- Avoid use in patients with moderate or severe hepatic impairment. (8.6 )
Recommended Dosage
The recommended dosages for PADCEV in combination with pembrolizumab or pembrolizumab and berahyaluronidase alfa-pmph, and PADCEV as a single agent are presented in Table 1 and Table 2 .
Administer PADCEV as an intravenous infusion over 30 minutes as recommended [see Instructions for Preparation and Administration (2.3 ) ]. Administer PADCEV prior to pembrolizumab or pembrolizumab and berahyaluronidase alfa-pmph if administering on the same day.
| Indication | Recommended PADCEV Dosage | Duration of Therapy |
|---|---|---|
Neoadjuvant and Adjuvant Muscle Invasive Bladder Cancer (MIBC) | PADCEV 1.25 mg/kg (up to a maximum of 125 mg for patients ≥100 kg) on Days 1 and 8 of a 21-day cycle. | Neoadjuvant: 3 cycles or until disease progression that precludes curative intent cystectomy or unacceptable toxicity. Adjuvant: 6 cycles or until disease recurrence or unacceptable toxicity. |
Locally advanced or metastatic Urothelial Cancer (mUC) | PADCEV 1.25 mg/kg (up to a maximum of 125 mg for patients ≥100 kg) on Days 1 and 8 of a 21-day cycle. | Until disease progression or unacceptable toxicity. |
| Indication | Recommended PADCEV Dosage | Duration of Therapy |
|---|---|---|
Locally advanced or metastatic Urothelial Cancer (mUC) | PADCEV 1.25 mg/kg (up to a maximum of 125 mg for patients ≥100 kg) on Days 1, 8, and 15 of a 28-day cycle. | Until disease progression or unacceptable toxicity. |
Dose Modifications
| Adverse Reaction | Severity Grade 1 is mild, Grade 2 is moderate, Grade 3 is severe, Grade 4 is life-threatening. | Dose Modification |
|---|---|---|
Skin Reactions [see Boxed Warning , Warnings and Precautions (5.1 )] | For persistent or recurrent Grade 2 skin reactions | Consider withholding until Grade ≤1, then resume treatment at the same dose level or dose reduce by one dose level. |
Grade 3 skin reactions | Withhold until Grade ≤1, then resume treatment at the same dose level or dose reduce by one dose level. | |
Suspected SJS or TEN | Immediately withhold, consult a specialist to confirm the diagnosis. If not SJS/TEN, see Grade 2-4 skin reactions. | |
Confirmed SJS or TEN; Grade 4 or recurrent Grade 3 skin reactions | Permanently discontinue. | |
Hyperglycemia [see Warnings and Precautions (5.2 )] | Blood glucose >250 mg/dL | Withhold until elevated blood glucose has improved to ≤250 mg/dL, then resume treatment at the same dose level. |
Pneumonitis/Interstitial Lung Disease (ILD) [see Warnings and Precautions (5.3 )] | Grade 2 | Withhold until Grade ≤1, then resume treatment at the same dose level or consider dose reduction by one dose level. |
Grade ≥3 | Permanently discontinue. | |
Peripheral Neuropathy [see Warnings and Precautions (5.4 )] | Grade 2 | Withhold until Grade ≤1, then resume treatment at the same dose level (if first occurrence). For a recurrence, withhold until Grade ≤1, then resume treatment reduced by one dose level. |
Grade ≥3 | Permanently discontinue. | |
Other Nonhematologic Toxicity [see Adverse Reactions (6 )] | Grade 3 | Withhold until Grade ≤1, then resume treatment at the same dose level or consider dose reduction by one dose level. |
Grade 4 | Permanently discontinue. | |
Hematologic Toxicity [see Adverse Reactions (6 )] | Grade 3, or Grade 2 thrombocytopenia | Withhold until Grade ≤1, then resume treatment at the same dose level or consider dose reduction by one dose level. |
Grade 4 | Withhold until Grade ≤1, then reduce dose by one dose level or discontinue treatment. |
Dose Reduction Schedule | Dose Level |
Starting dose | 1.25 mg/kg up to 125 mg |
First dose reduction | 1 mg/kg up to 100 mg |
Second dose reduction | 0.75 mg/kg up to 75 mg |
Third dose reduction | 0.5 mg/kg up to 50 mg |
Instructions for Preparation and Administration
- Administer PADCEV as an intravenous infusion only.
- PADCEV is a hazardous drug. Follow applicable special handling and disposal procedures. 1
Prior to administration, the PADCEV vial is reconstituted with Sterile Water for Injection (SWFI). The reconstituted solution is subsequently diluted in an intravenous infusion bag containing either 5% Dextrose Injection, USP, 0.9% Sodium Chloride Injection, USP, or Lactated Ringer’s Injection, USP.
Reconstitution in Single-Dose Vial
- Follow procedures for proper handling and disposal of anticancer drugs.
- Use appropriate aseptic technique for reconstitution and preparation of dosing solutions.
- Calculate the recommended dose based on the patient’s weight to determine the number and strength (20 mg or 30 mg) of vials needed.
- Reconstitute each vial as follows and, if possible, direct the stream of SWFI along the walls of the vial and not directly onto the lyophilized powder:
- 20 mg vial: Add 2.3 mL of SWFI, resulting in 10 mg/mL PADCEV.
- 30 mg vial: Add 3.3 mL of SWFI, resulting in 10 mg/mL PADCEV.
- Slowly swirl each vial until the contents are completely dissolved. Allow the reconstituted vial(s) to settle for at least 1 minute until the bubbles are gone. DO NOT SHAKE THE VIAL. Do not expose to direct sunlight.
- Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. The reconstituted solution should be clear to slightly opalescent, colorless to light yellow, and free of visible particles. Discard any vial with visible particles or discoloration.
- Based upon the calculated dose amount, the reconstituted solution from the vial(s) should be added to the infusion bag immediately. This product does not contain a preservative. If not used immediately, reconstituted vials may be stored for up to 24 hours in refrigeration at 2°C to 8°C (36°F to 46°F). DO NOT FREEZE. Discard unused vials with reconstituted solution beyond the recommended storage time.
Dilution in Infusion Bag
- Withdraw the calculated dose amount of reconstituted solution from the vial(s) and transfer into an infusion bag.
- Dilute PADCEV with either 5% Dextrose Injection, 0.9% Sodium Chloride Injection, or Lactated Ringer's Injection. The infusion bag size should allow enough diluent to achieve a final concentration of 0.3 mg/mL to 4 mg/mL PADCEV.
- Mix diluted solution by gentle inversion. DO NOT SHAKE THE BAG. Do not expose to direct sunlight.
- Visually inspect the infusion bag for any particulate matter or discoloration prior to use. The reconstituted solution should be clear to slightly opalescent, colorless to light yellow, and free of visible particles. DO NOT USE the infusion bag if particulate matter or discoloration is observed.
- Discard any unused portion left in the single-dose vials.
Administration
- Immediately administer the infusion over 30 minutes through an intravenous line.
- If the infusion is not administered immediately, the prepared infusion bag should not be stored longer than 8 hours at 2°C to 8°C (36°F to 46°F). DO NOT FREEZE.
DO NOT administer PADCEV as an intravenous push or bolus.
DO NOT mix PADCEV with, or administer as an infusion with, other medicinal products.
DOSAGE FORMS AND STRENGTHS
For Injection: 20 mg and 30 mg of enfortumab vedotin-ejfv as a white to off-white lyophilized powder in a single-dose vial for reconstitution.
USE IN SPECIFIC POPULATIONS
- Lactation: Advise women not to breastfeed. (8.2 )
Pregnancy
Risk Summary
Based on the mechanism of action and findings in animals, PADCEV can cause fetal harm when administered to a pregnant woman [see Clinical Pharmacology (12.1 )] . There are no available human data on PADCEV use in pregnant women to inform a drug-associated risk. In an animal reproduction study, administration of enfortumab vedotin-ejfv to pregnant rats during organogenesis caused maternal toxicity, embryo-fetal lethality, structural malformations, and skeletal anomalies at maternal exposures similar to the exposures at the recommended human dose of 1.25 mg/kg (see Data ) . Advise patients of the potential risk to the fetus.
The background risk of major birth defects and miscarriage for the indicated population is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2%-4% and 15%-20%, respectively.
Data
Animal Data
In a rat pilot embryo-fetal development study, administration of enfortumab vedotin-ejfv on gestation day 6 and 13 during the period of organogenesis resulted in a complete litter loss in all pregnant rats at the maternally toxic dose of 5 mg/kg (approximately 3 times the exposure at the recommended human dose). A dose of 2 mg/kg (similar to the exposure at the recommended human dose) resulted in maternal toxicity, embryo-fetal lethality, and structural malformations that included gastroschisis, malrotated hindlimb, absent forepaw, malpositioned internal organs, and fused cervical arch. Additionally, skeletal anomalies (asymmetric, fused, incompletely ossified, and misshapen sternebrae, misshapen cervical arch, and unilateral ossification of the thoracic centra) and decreased fetal weight were observed.
Lactation
Risk Summary
There are no data on the presence of enfortumab vedotin-ejfv in human milk, the effects on the breastfed child, or the effects on milk production. Because of the potential for serious adverse reactions in a breastfed child, advise lactating women not to breastfeed during treatment with PADCEV and for 3 weeks after the last dose.
Females and Males of Reproductive Potential
Pregnancy Testing
Verify pregnancy status in females of reproductive potential prior to initiating PADCEV treatment [see Use in Specific Populations (8.1 )] .
Contraception
Females
PADCEV can cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1 )] . Advise females of reproductive potential to use effective contraception during treatment with PADCEV and for 2 months after the last dose.
Males
Advise male patients with female partners of reproductive potential to use effective contraception during treatment with PADCEV and for 4 months after the last dose.
Infertility
Females
Based on findings in animal studies with MMAE-containing antibody-drug conjugates (ADCs), PADCEV may impair female fertility. The effect on fertility is reversible [see Nonclinical Toxicology (13.1 )] .
Males
Based on findings from animal studies, PADCEV may impair male fertility [see Nonclinical Toxicology (13.1 )] .
Pediatric Use
Safety and effectiveness of PADCEV in pediatric patients have not been established.
Geriatric Use
Of the 167 patients treated with PADCEV in combination with intravenous pembrolizumab for the treatment of MIBC, 37% (n=61) were 65-74 years and 46% (n=77) were 75 years or older. Of the 564 patients treated with PADCEV in combination with intravenous pembrolizumab for the treatment of locally advanced or mUC, 44% (n=247) were 65‑74 years and 26% (n=144) were 75 years or older. Of the 720 patients treated with PADCEV as a single agent in clinical trials, 39% (n=282) were 65‑74 years and 24% (n=170) were 75 years or older. No overall differences in effectiveness were observed between patients 65 years of age or older and younger patients.
Patients 75 years of age or older treated with PADCEV in combination with intravenous pembrolizumab for the treatment of MIBC experienced a higher incidence of fatal adverse reactions than younger patients. The incidence of fatal adverse reactions was 4% in patients younger than 75 and 12% in patients 75 years or older.
Patients 75 years of age or older treated with PADCEV in combination with intravenous pembrolizumab for the treatment of locally advanced or mUC experienced a higher incidence of fatal adverse reactions than younger patients. The incidence of fatal adverse reactions was 4% in patients younger than 75 and 7% in patients 75 years or older.
Patients 75 years of age or older treated with PADCEV as a single agent experienced a higher incidence of fatal adverse reactions than younger patients. The incidence of fatal adverse reactions was 6% in patients younger than 75 years, and 11% in patients 75 years or older.
No significant difference was observed in the pharmacokinetics of PADCEV between patients 65 years and older and younger patients [see Clinical Pharmacology (12.3 )].
Hepatic Impairment
Avoid the use of PADCEV in patients with moderate or severe hepatic impairment (total bilirubin >1.5 × ULN and any AST). PADCEV has only been studied in a limited number of patients with moderate or severe hepatic impairment [see Clinical Pharmacology (12.3 )] . In another ADC that contains MMAE, the frequency of ≥ Grade 3 adverse reactions and deaths was greater in patients with moderate (Child-Pugh B) or severe (Child-Pugh C) hepatic impairment compared to patients with normal hepatic function.
CONTRAINDICATIONS
None.
WARNINGS AND PRECAUTIONS
- Hyperglycemia: Diabetic ketoacidosis may occur in patients with and without preexisting diabetes mellitus, which may be fatal. Closely monitor blood glucose levels in patients with, or at risk for, diabetes mellitus or hyperglycemia. Withhold PADCEV if blood glucose is >250 mg/dL. (2.2 , 5.2 )
- Pneumonitis/Interstitial Lung Disease (ILD): Severe, life-threatening or fatal pneumonitis/ILD may occur. Withhold PADCEV for Grade 2 pneumonitis/ILD and consider dose reduction. Permanently discontinue PADCEV for Grade 3 or 4 pneumonitis/ILD. (2.2 , 5.3 )
- Peripheral Neuropathy: Monitor patients for new or worsening peripheral neuropathy and consider dose interruption, dose reduction, or discontinuation of PADCEV. (2.2 , 5.4 )
- Ocular Disorders: Ocular disorders, including vision changes, may occur. Monitor patients for signs or symptoms of ocular disorders. Consider prophylactic artificial tears for dry eyes and treatment with ophthalmic topical steroids after an ophthalmic exam. Consider dose interruption or dose reduction of PADCEV when symptomatic ocular disorders occur. (5.5 )
- Infusion Site Extravasation: Ensure adequate venous access prior to administration. Monitor the infusion site during PADCEV administration and stop the infusion immediately for suspected extravasation. (5.6 )
- Embryo-Fetal Toxicity: PADCEV can cause fetal harm. Advise of the potential risk to a fetus and to use effective contraception. (5.7 , 8.1 , 8.3 )
Skin Reactions
Severe cutaneous adverse reactions, including fatal cases of SJS or TEN occurred in patients treated with PADCEV. SJS and TEN occurred predominantly during the first cycle of treatment but may occur later.
Skin reactions occurred in 61% (all grades) of the 167 patients treated with PADCEV in combination with intravenous pembrolizumab for the treatment of MIBC in clinical trials. The majority of the skin reactions that occurred with combination therapy included rash and maculo-papular rash. Grade 3-4 skin reactions occurred in 10% of patients (Grade 3: 9%, Grade 4: 1.2%), including rash, maculo-papular rash, toxic skin eruption, dermatitis exfoliative generalized, erythema, exfoliative rash, skin toxicity, toxic epidermal necrolysis, and toxic erythema of chemotherapy. A fatal reaction of toxic epidermal necrolysis occurred in one patient (0.6%). The median time to onset of severe skin reactions was 0.6 months (range: 0.2 to 8.8 months). Skin reactions led to discontinuation of PADCEV in 10% of patients [see Adverse Reactions (6.1 )] . Of the patients who experienced a skin reaction and had data regarding resolution (n=102), 83% had complete resolution and 17% had residual skin reactions at their last evaluation. Of the patients with residual skin reactions at last evaluation, 29% (5/17) had Grade ≥2 skin reactions.
Skin reactions occurred in 70% (all grades) of the 564 patients treated with PADCEV in combination with intravenous pembrolizumab for the treatment of locally advanced or mUC in clinical trials. When PADCEV was given in combination with intravenous pembrolizumab, the incidence of skin reactions, including severe events, occurred at a higher rate compared to PADCEV as a single agent. The majority of the skin reactions that occurred with combination therapy included maculo-papular rash, macular rash, and papular rash. Grade 3-4 skin reactions occurred in 17% of patients (Grade 3: 16%, Grade 4: 1%), including maculo-papular rash, bullous dermatitis, dermatitis, exfoliative dermatitis, pemphigoid, rash, erythematous rash, macular rash, and papular rash. A fatal reaction of bullous dermatitis occurred in one patient (0.2%). The median time to onset of severe skin reactions was 1.7 months (range: 0.1 to 17.2 months). Skin reactions led to discontinuation of PADCEV in 6% of patients [see Adverse Reactions (6.1 )] . Of the patients who experienced a skin reaction and had data regarding resolution (n=391), 59% had complete resolution and 41% had residual skin reactions at their last evaluation. Of the patients with residual skin reactions at last evaluation, 27% (43/159) had Grade ≥2 skin reactions.
Skin reactions occurred in 58% (all grades) of the 720 patients treated with PADCEV as a single agent in clinical trials. Twenty-three percent (23%) of patients had maculo-papular rash and 34% had pruritus. Grade 3-4 skin reactions occurred in 14% of patients, including maculo-papular rash, erythematous rash, rash or drug eruption, symmetrical drug-related intertriginous and flexural exanthema (SDRIFE), bullous dermatitis, exfoliative dermatitis, and palmar-plantar erythrodysesthesia. The median time to onset of severe skin reactions was 0.6 months (range: 0.1 to 8 months). Among patients experiencing a skin reaction leading to dose interruption who then restarted PADCEV (n=75), 24% of patients restarting at the same dose and 24% of patients restarting at a reduced dose experienced recurrent severe skin reactions. Skin reactions led to discontinuation of PADCEV in 3.1% of patients [see Adverse Reactions (6.1 )] . Of the patients who experienced a skin reaction and had data regarding resolution (n=328), 58% had complete resolution and 42% had residual skin reactions at their last evaluation. Of the patients with residual skin reactions at last evaluation, 39% (53/137) had Grade ≥2 skin reactions.
Monitor patients closely throughout treatment for skin reactions. Consider topical corticosteroids and antihistamines, as clinically indicated.
For persistent or recurrent Grade 2 skin reactions, consider withholding PADCEV until Grade ≤1. Withhold PADCEV and refer for specialized care for suspected SJS, TEN or for Grade 3 skin reactions.
Permanently discontinue PADCEV in patients with confirmed SJS or TEN; or Grade 4 or recurrent Grade 3 skin reactions [see Dosage and Administration (2.2 )] .
Hyperglycemia
Hyperglycemia and diabetic ketoacidosis (DKA), including fatal events, occurred in patients with and without pre‑existing diabetes mellitus, treated with PADCEV.
Patients with baseline hemoglobin A1C ≥8% were excluded from clinical trials.
In clinical trials of PADCEV as a single agent, 17% of the 720 patients treated with PADCEV developed hyperglycemia of any grade; 7% of patients developed Grade 3-4 hyperglycemia (Grade 3: 6.5%, Grade 4: 0.6%). Fatal events of hyperglycemia and diabetic ketoacidosis occurred in one patient each (0.1%). The incidence of Grade 3-4 hyperglycemia increased consistently in patients with higher body mass index and in patients with higher baseline A1C. The median time to onset of hyperglycemia was 0.5 months (range: 0 to 20 months). Hyperglycemia led to discontinuation of PADCEV in 0.7% of patients [see Adverse Reactions (6.1 )] . Five percent (5%) of patients required initiation of insulin therapy for treatment of hyperglycemia. Of the patients who initiated insulin therapy for treatment of hyperglycemia, 66% (23/35) discontinued insulin by the time of last evaluation.
Closely monitor blood glucose levels in patients with, or at risk for, diabetes mellitus or hyperglycemia.
If blood glucose is elevated (>250 mg/dL), withhold PADCEV [see Dosage and Administration (2.2 )] .
Pneumonitis/Interstitial Lung Disease (ILD)
Severe, life-threatening or fatal pneumonitis/ILD occurred in patients treated with PADCEV.
When PADCEV was given in combination with intravenous pembrolizumab for the treatment of MIBC, 4.2% of the 167 patients treated with combination therapy had pneumonitis/ILD of any grade. All events were Grade 1-2. The median time to onset of any grade pneumonitis/ILD was 2.5 months (range: 1.9 to 9.7 months).
When PADCEV was given in combination with intravenous pembrolizumab for the treatment of locally advanced or mUC, 10% of the 564 patients treated with combination therapy had pneumonitis/ILD of any grade and 4% had Grade 3-4. A fatal event of pneumonitis/ILD occurred in two patients (0.4%). The incidence of pneumonitis/ILD, including severe events, occurred at a higher rate when PADCEV was given in combination with intravenous pembrolizumab compared to PADCEV as a single agent. The median time to onset of any grade pneumonitis/ILD was 4 months (range: 0.3 to 26 months).
In clinical trials of PADCEV as a single agent, 3% of the 720 patients treated with PADCEV had pneumonitis/ILD of any grade and 0.8% had Grade 3-4. The median time to onset of any grade pneumonitis/ILD was 2.9 months (range: 0.6 to 6 months).
Monitor patients for signs and symptoms indicative of pneumonitis/ILD such as hypoxia, cough, dyspnea or interstitial infiltrates on radiologic exams. Evaluate and exclude infectious, neoplastic and other causes for such signs and symptoms through appropriate investigations.
Withhold PADCEV for patients who develop Grade 2 pneumonitis/ILD and consider dose reduction. Permanently discontinue PADCEV in all patients with Grade 3 or 4 pneumonitis/ILD [see Dosage and Administration (2.2 )] .
Peripheral Neuropathy
When PADCEV was given in combination with intravenous pembrolizumab for the treatment of MIBC, 39% of the 167 patients treated with combination therapy had peripheral neuropathy of any grade, 12% had Grade 2 neuropathy, and 3% had Grade 3 neuropathy. The median time to onset of Grade ≥2 peripheral neuropathy was 4.7 months (range: 0.2 to 11 months) [see Adverse Reactions (6.1 )] . Of the patients who experienced neuropathy and had data regarding resolution (n=65), 32% had complete resolution, and 68% of patients had residual neuropathy at last evaluation. Of the patients with residual neuropathy at last evaluation, 27% (12/44) had Grade ≥2 neuropathy.
When PADCEV was given in combination with intravenous pembrolizumab for the treatment of locally advanced or mUC, 67% of the 564 patients treated with combination therapy had peripheral neuropathy of any grade, 36% had Grade 2 neuropathy, and 7% had Grade 3 neuropathy. The incidence of peripheral neuropathy occurred at a higher rate when PADCEV was given in combination with intravenous pembrolizumab compared to PADCEV as a single agent. The median time to onset of Grade ≥2 peripheral neuropathy was 6 months (range: 0.3 to 25 months) [see Adverse Reactions (6.1 )] . Of the patients who experienced neuropathy and had data regarding resolution (n=373), 13% had complete resolution, and 87% of patients had residual neuropathy at last evaluation. Of the patients with residual neuropathy at last evaluation, 45% (146/326) had Grade ≥2 neuropathy.
Peripheral neuropathy occurred in 53% of the 720 patients treated with PADCEV as a single agent in clinical trials including 38% with sensory neuropathy, 8% with muscular weakness, and 7% with motor neuropathy. Thirty percent of patients experienced Grade 2 reactions and 5% experienced Grade 3-4 reactions. Peripheral neuropathy occurred in patients treated with PADCEV with or without preexisting peripheral neuropathy. The median time to onset of Grade ≥2 peripheral neuropathy was 4.9 months (range: 0.1 to 20 months). Neuropathy led to treatment discontinuation in 6% of patients [see Adverse Reactions (6.1 )] . Of the patients who experienced neuropathy who had data regarding resolution (n=296), 11% had complete resolution, and 89% had residual neuropathy at the time of their last evaluation. Of the patients with residual neuropathy at last evaluation, 50% (132/262) had Grade ≥2 neuropathy.
Monitor patients for symptoms of new or worsening peripheral neuropathy and consider dose interruption or dose reduction of PADCEV when peripheral neuropathy occurs.
Permanently discontinue PADCEV in patients who develop Grade > 3 peripheral neuropathy [see Dosage and Administration (2.2 )] .
Ocular Disorders
Ocular disorders were reported in 40% of the 384 patients treated with PADCEV as a single agent in clinical trials in which ophthalmologic exams were scheduled. The majority of these events involved the cornea and included events associated with dry eye such as keratitis, blurred vision, increased lacrimation, conjunctivitis, limbal stem cell deficiency, and keratopathy.
Dry eye symptoms occurred in 30% of patients, and blurred vision occurred in 10% of patients, during treatment with PADCEV. The median time to onset to symptomatic ocular disorder was 1.7 months (range: 0 to 30.6 months). Monitor patients for ocular disorders. Consider artificial tears for prophylaxis of dry eyes and ophthalmologic evaluation if ocular symptoms occur or do not resolve. Consider treatment with ophthalmic topical steroids, if indicated after an ophthalmic exam. Consider dose interruption or dose reduction of PADCEV for symptomatic ocular disorders.
Infusion Site Extravasation
Skin and soft tissue reactions secondary to extravasation have been observed after administration of PADCEV. Of the 720 patients treated with PADCEV as a single agent in clinical trials, 1% of patients experienced skin and soft tissue reactions, including 0.3% who experienced Grade 3-4 reactions. Reactions may be delayed. Erythema, swelling, increased temperature, and pain worsened until 2-7 days after extravasation and resolved within 1-4 weeks of peak. Two patients (0.3%) developed extravasation reactions with secondary cellulitis, bullae, or exfoliation. Ensure adequate venous access prior to starting PADCEV and monitor for possible extravasation during administration. If extravasation occurs, stop the infusion and monitor for adverse reactions.
Embryo-Fetal Toxicity
Based on the mechanism of action and findings in animals, PADCEV can cause fetal harm when administered to a pregnant woman. In animal reproduction studies, administration of enfortumab vedotin-ejfv to pregnant rats during the period of organogenesis caused maternal toxicity, embryo-fetal lethality, structural malformations and skeletal anomalies at maternal exposures similar to the clinical exposures at the recommended human dose of 1.25 mg/kg.
Advise patients of the potential risk to the fetus. Advise female patients of reproductive potential to use effective contraception during treatment with PADCEV and for 2 months after the last dose. Advise male patients with female partners of reproductive potential to use effective contraception during treatment with PADCEV and for 4 months after the last dose [see Use in Specific Populations (8.1 , 8.3 ) and Clinical Pharmacology (12.1 )] .
ADVERSE REACTIONS
The following serious adverse reactions are described elsewhere in the labeling:
- Skin Reactions [see Boxed Warning , Warnings and Precautions (5.1 )]
- Hyperglycemia [see Warnings and Precautions (5.2 )]
- Pneumonitis/Interstitial Lung Disease (ILD) [see Warnings and Precautions (5.3 )]
- Peripheral Neuropathy [see Warnings and Precautions (5.4 )]
- Ocular Disorders [see Warnings and Precautions (5.5 )]
- Infusion Site Extravasation [see Warnings and Precautions (5.6 )]
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety population described in the WARNINGS AND PRECAUTIONS reflect exposure to PADCEV 1.25 mg/kg in combination with intravenous pembrolizumab for the treatment of MIBC in 167 patients in EV-303 (NCT03924895) and for the treatment of locally advanced or mUC in 564 patients in EV-302 (NCT04223856) and EV-103 (NCT03288545); PADCEV as a single agent at 1.25 mg/kg in 720 patients in EV-301 (NCT03474107), EV-201 (NCT03219333), EV-203 (NCT04995419), EV-101 (NCT02091999), and EV-102 (NCT03070990). Ocular disorders reflect 384 patients in EV‑201, EV-101, and EV-102.
Among 167 patients receiving PADCEV in combination with intravenous pembrolizumab for the treatment of MIBC, the most common (≥20%) adverse reactions, including laboratory abnormalities, were increased glucose, decreased hemoglobin, increased aspartate aminotransferase, rash, increased alanine aminotransferase, fatigue, pruritus, increased creatinine, decreased sodium, decreased lymphocytes, peripheral neuropathy, increased potassium, alopecia, dysgeusia, diarrhea, decreased appetite, constipation, nausea, decreased phosphate, urinary tract infection, dry eye, and decreased weight.
Among 564 patients receiving PADCEV in combination with intravenous pembrolizumab for the treatment of locally advanced or mUC, 59% were exposed to PADCEV for ≥6 months, and 24% were exposed for ≥12 months. In this pooled population, the most common (≥20%) adverse reactions, including laboratory abnormalities, were increased aspartate aminotransferase, increased creatinine, rash, increased glucose, peripheral neuropathy, increased lipase, decreased lymphocytes, increased alanine aminotransferase, decreased hemoglobin, fatigue, decreased sodium, decreased phosphate, decreased albumin, pruritus, diarrhea, alopecia, decreased weight, decreased appetite, increased urate, decreased neutrophils, decreased potassium, dry eye, nausea, constipation, increased potassium, dysgeusia, urinary tract infection, and decreased platelets.
Among 720 patients receiving PADCEV as a single agent, 37% were exposed for ≥6 months, and 14% were exposed for ≥12 months. In this pooled population, the most common (≥20%) adverse reactions, including laboratory abnormalities, were increased glucose, increased aspartate aminotransferase, decreased lymphocytes, increased creatinine, rash, fatigue, peripheral neuropathy, decreased albumin, decreased hemoglobin, alopecia, decreased appetite, decreased neutrophils, decreased sodium, increased alanine aminotransferase, decreased phosphate, diarrhea, nausea, pruritus, increased urate, dry eye, dysgeusia, constipation, increased lipase, decreased weight, decreased platelets, abdominal pain, and dry skin.
The data described in the following section reflects exposure to PADCEV in combination with intravenous pembrolizumab from EV‑302, the dose escalation cohort, Cohort A and Cohort K of EV-103, and EV-303. Patients received PADCEV 1.25 mg/kg in combination with intravenous pembrolizumab until disease progression or unacceptable toxicity.
The data described in the following section also reflects exposure to PADCEV as a single agent from an open-label, randomized, trial (EV‑301) and Cohort 1 and Cohort 2 of an open-label, single arm, two cohort trial (EV-201). Patients received PADCEV 1.25 mg/kg until disease progression or unacceptable toxicity.
Neoadjuvant and Adjuvant Treatment of Cisplatin-Ineligible Patients with MIBC
EV-303
The safety of PADCEV in combination with intravenous pembrolizumab as neoadjuvant treatment and continued after radical cystectomy (RC) as adjuvant treatment was evaluated in an open-label, randomized, multicenter trial (EV-303) in patients with previously untreated MIBC who were ineligible for or declined cisplatin-based chemotherapy. Patients received PADCEV 1.25 mg/kg in combination with intravenous pembrolizumab (n=167) before and after RC with pelvic lymph node dissection (PLND) or RC with PLND alone (n=159) [see Clinical Studies (14 )] .
For the 167 patients who received PADCEV in the neoadjuvant phase, the median duration of exposure to PADCEV was 1.6 months (range: 0.03 to 2.8 months) and the median number of cycles of PADCEV was 3 (range: 1, 3) in the neoadjuvant phase. For the 92 patients who received PADCEV in the adjuvant phase, the median duration of exposure to PADCEV was 3.7 months (range: 0.03 to 7.6 months) and the median number of cycles of PADCEV was 6 (range: 1, 6) in the adjuvant phase. Across the combined neoadjuvant and adjuvant phases (n=167), the median number of cycles of PADCEV was 5 (range: 1, 9) out of a planned 9 cycles.
Table 5 summarizes the most common (≥20%) adverse reactions in EV-303.
| Adverse Reaction | PADCEV in combination with intravenous pembrolizumab before and after RC with PLND n=167 | RC with PLND alone n=159 | ||
|---|---|---|---|---|
| All Grades % | Grade 3-4 % | All Grades % | Grade 3-4 % | |
Skin and subcutaneous tissue disorders | ||||
Rash Includes: multiple terms. | 54 | 7 | 1.3 | 0 |
Pruritus | 47 | 3 | 0 | 0 |
Alopecia | 35 | 0.6 | 0 | 0 |
General disorders and administration site conditions | ||||
Fatigue | 47 | 4.2 | 6 | 0.6 |
Nervous system disorders | ||||
Peripheral neuropathy | 39 | 3 | 1.9 | 0 |
Dysgeusia | 35 | 0 | 0 | 0 |
Gastrointestinal disorders | ||||
Diarrhea | 34 | 5 | 3.1 | 1.3 |
Constipation | 28 | 1.8 | 8 | 0 |
Nausea | 26 | 1.2 | 8 | 0.6 |
Metabolism and nutrition disorders | ||||
Decreased appetite | 28 | 0.6 | 1.9 | 0 |
Infections and infestations | ||||
Urinary tract infection | 24 | 12 | 13 | 11 |
Eye disorders | ||||
Dry eye | 21 | 0 | 0 | 0 |
Investigations | ||||
Decreased weight | 20 | 0 | 3.1 | 0 |
Clinically relevant adverse reactions (<20%) include dry skin (15%), hypothyroidism (14%), vomiting (9%), pneumonitis/ILD (4.2%), skin hyperpigmentation (3%), infusion site extravasation (1.2%), and myasthenia gravis and myositis (0.6% each).
| Laboratory Abnormality | PADCEV in combination with intravenous pembrolizumab before and after RC with PLND | RC with PLND alone | ||
|---|---|---|---|---|
| All Grades The denominator used to calculate the rate of PADCEV in combination with intravenous pembrolizumab was 167 and the denominator used to calculate the rate for RC and PLND alone varied from 110 to 121 based on the number of patients with a baseline value and at least one post-treatment value. % | Grade 3-4 % | All Grades % | Grade 3-4 % | |
Chemistry | ||||
Increased glucose | 72 | 12 | 24 | 1.7 |
Increased aspartate aminotransferase | 55 | 6 | 11 | 1.8 |
Increased alanine aminotransferase | 53 | 4.8 | 13 | 0.9 |
Increased creatinine | 47 | 8 | 31 | 2.5 |
Decreased sodium | 44 | 13 | 18 | 7 |
Increased potassium | 39 | 7 | 20 | 6 |
Decreased phosphate | 26 | 6 | 1.8 | 0 |
Hematology | ||||
Decreased hemoglobin | 60 | 13 | 48 | 8 |
Decreased lymphocytes | 40 | 8 | 17 | 1.7 |
Neoadjuvant Phase of EV-303
A total of 167 patients received at least one dose of PADCEV in combination with intravenous pembrolizumab as neoadjuvant treatment before receiving RC.
In the neoadjuvant phase, serious adverse reactions occurred in 27% of patients receiving PADCEV in combination with intravenous pembrolizumab. The most frequent (≥2%) serious adverse reactions were urinary tract infection (3.6%) and hematuria (2.4%). Fatal adverse reactions occurred in 1.2% of patients including myasthenia gravis and toxic epidermal necrolysis (0.6% each). Additional fatal adverse reactions were reported in 2.7% of patients in the post-surgery phase before adjuvant treatment started, including sepsis and intestinal obstruction (1.4% each).
Adverse reactions leading to discontinuation of PADCEV in the neoadjuvant phase occurred in 22% of patients. The most common adverse reactions (≥1%) leading to discontinuation of PADCEV were rash (4.8%), peripheral neuropathy (2.4%), and diarrhea, dysgeusia, fatigue, pruritus, and toxic epidermal necrolysis (1.2% each).
Adverse reactions leading to dose interruption of PADCEV in the neoadjuvant phase occurred in 29% of patients. The most common adverse reactions (≥2%) leading to dose interruption of PADCEV were rash (8%), neutropenia (3.6%), hyperglycemia (3%), and fatigue and peripheral neuropathy (2.4% each).
Adverse reactions leading to dose reduction of PADCEV in the neoadjuvant phase occurred in 13% of patients. The most common adverse reactions (≥1%) leading to dose reduction of PADCEV were rash (4.8%), pruritus (1.8%), and peripheral neuropathy, increase alanine aminotransferase, increased aspartate aminotransferase, decreased appetite, fatigue, neutropenia, and decreased weight (1.2% each).
Of the 167 patients in the PADCEV in combination with intravenous pembrolizumab arm who received neoadjuvant treatment, 7 (4.2%) patients did not receive surgery due to adverse reactions. The adverse reactions that led to cancellation of surgery were acute myocardial infarction, bile duct cancer, colon cancer, respiratory distress, urinary tract infection and the deaths due to myasthenia gravis and toxic epidermal necrolysis (0.6% each).
Of the 146 patients who received neoadjuvant treatment with PADCEV in combination with intravenous pembrolizumab and underwent RC, 6 (4.1%) patients experienced delay of surgery (defined as time from last neoadjuvant treatment to surgery exceeding 8 weeks) due to adverse reactions.
Adjuvant Phase of EV-303
Patients who did not proceed to surgery were ineligible for adjuvant treatment. Of the 149 patients who underwent surgery, 100 patients received adjuvant treatment with PADCEV in combination with intravenous pembrolizumab. Of the 49 patients who did not receive adjuvant treatment, discontinuation of treatment with PADCEV in combination with intravenous pembrolizumab prior to the adjuvant phase was due to an adverse event in 21 patients.
In the adjuvant phase, serious adverse reactions occurred in 43% of patients receiving PADCEV in combination with intravenous pembrolizumab. The most frequent (≥2%) serious adverse reactions were urinary tract infection (8%), acute kidney injury and pyelonephritis (5% each), urosepsis (4%), and hypokalemia, intestinal obstruction, and sepsis (2% each). Fatal adverse reactions occurred in 7% of patients, including urosepsis, hemorrhage intracranial, death, myocardial infarction, multiple organ dysfunction syndrome, and pneumonia pseudomonal (1% each).
Adverse reactions leading to discontinuation of PADCEV in the adjuvant phase occurred in 26% of patients. The most common adverse reactions (≥2%) leading to discontinuation of PADCEV were peripheral neuropathy (5%) and rash (4%).
Adverse reactions leading to dose interruption of PADCEV in the adjuvant phase occurred in 36% of patients. The most common adverse reactions (≥2%) leading to dose interruption of PADCEV were rash (6%), diarrhea and urinary tract infection (5% each), fatigue (4%), pruritus (3%), and peripheral neuropathy and pyelonephritis (2% each).
Adverse reactions leading to dose reduction of PADCEV in the adjuvant phase occurred in 7% of patients. The most common adverse reaction (≥2%) leading to dose reduction of PADCEV was weight decreased (2%).
Previously Untreated Locally Advanced or mUC
EV-302
The safety of PADCEV in combination with intravenous pembrolizumab was evaluated in an open-label, randomized, multicenter trial (EV-302) in patients with locally advanced or mUC. Patients received either PADCEV 1.25 mg/kg and pembrolizumab (n=440) or gemcitabine and platinum chemotherapy (either cisplatin or carboplatin) (n=433). Among patients who received PADCEV and pembrolizumab, the median duration of exposure for PADCEV was 7 months (range: 0.3 to 31.9 months).
Serious adverse reactions occurred in 50% of patients treated with PADCEV in combination with intravenous pembrolizumab. The most common serious adverse reactions (≥2%) were rash (6%), acute kidney injury (5%), pneumonitis/ILD (4.5%), urinary tract infection (3.6%), diarrhea (3.2%), pneumonia (2.3%), pyrexia (2%), and hyperglycemia (2%).
Fatal adverse reactions occurred in 3.9% of patients treated with PADCEV in combination with intravenous pembrolizumab including acute respiratory failure (0.7%), pneumonia (0.5%), and pneumonitis/ILD (0.2%).
Adverse reactions leading to discontinuation of PADCEV occurred in 35% of patients. The most common adverse reactions (≥2%) leading to discontinuation of PADCEV were peripheral neuropathy (15%), rash (4.1%), and pneumonitis/ILD (2.3%).
Adverse reactions leading to dose interruption of PADCEV occurred in 73% of patients. The most common adverse reactions (≥2%) leading to dose interruption of PADCEV were peripheral neuropathy (22%), rash (16%), COVID-19 (10%), diarrhea (5%), pneumonitis/ILD (4.8%), fatigue (3.9%), hyperglycemia (3.6%), increased alanine aminotransferase (3%), and pruritus (2.5%).
Adverse reactions leading to dose reduction of PADCEV occurred in 42% of patients. The most common adverse reactions (≥2%) leading to dose reduction of PADCEV were rash (16%), peripheral neuropathy (13%), and fatigue (2.7%).
Table 7 summarizes the most common (≥15%) adverse reactions in EV-302.
| Adverse Reaction | PADCEV in combination with intravenous pembrolizumab n=440 | Chemotherapy n=433 | ||
|---|---|---|---|---|
| All Grades % | Grade 3-4 % | All Grades % | Grade 3-4 % | |
Skin and subcutaneous tissue disorders | ||||
Rash Includes: multiple terms. | 68 | 15 | 15 | 0 |
Pruritus | 41 | 1.1 | 7 | 0 |
Alopecia | 35 | 0.5 | 8 | 0.2 |
Dry skin | 17 | 0.2 | 1 | 0 |
General disorders and administration site conditions | ||||
Fatigue | 51 | 6 | 57 | 7 |
Pyrexia | 18 | 0.7 | 16 | 1.2 |
Nervous system disorders | ||||
Peripheral neuropathy | 67 | 8 | 14 | 0 |
Dysgeusia | 21 | 0 | 9 | 0 |
Metabolism and nutrition disorders | ||||
Decreased appetite | 33 | 1.8 | 26 | 1.8 |
Gastrointestinal disorders | ||||
Diarrhea | 38 | 4.5 | 16 | 1.4 |
Nausea | 26 | 1.6 | 41 | 2.8 |
Constipation | 26 | 0 | 34 | 0.7 |
Investigations | ||||
Decreased weight | 33 | 3.6 | 9 | 0.2 |
Eye disorders | ||||
Dry eye | 24 | 0 | 2.1 | 0 |
Infections and infestations | ||||
Urinary tract infection | 21 | 5 | 19 | 8 |
Clinically relevant adverse reactions (<15%) include vomiting (12%), pneumonitis/ILD and hypothyroidism (10% each), blurred vision and skin hyperpigmentation (6% each), infusion site extravasation (1.8%), and myositis (0.5%).
| Laboratory Abnormality | PADCEV in combination with intravenous pembrolizumab | Chemotherapy | ||
|---|---|---|---|---|
| All Grades The denominator used to calculate the rate varied from 407 to 439 based on the number of patients with a baseline value and at least one post-treatment value. % | Grade 3-4 % | All Grades % | Grade 3-4 % | |
Chemistry | ||||
Increased aspartate aminotransferase | 75 | 5 | 39 | 3 |
Increased creatinine | 71 | 3 | 68 | 3 |
Increased glucose | 66 | 14 | 54 | 5 |
Increased alanine aminotransferase | 59 | 5 | 49 | 3 |
Decreased sodium | 46 | 13 | 47 | 13 |
Decreased phosphate | 44 | 9 | 36 | 9 |
Decreased albumin | 39 | 2 | 35 | 0.5 |
Decreased potassium | 26 | 5 | 16 | 3 |
Increased potassium | 24 | 1 | 36 | 4 |
Increased calcium | 21 | 1 | 14 | 0.2 |
Hematology | ||||
Decreased lymphocytes | 58 | 15 | 59 | 17 |
Decreased hemoglobin | 53 | 7 | 89 | 33 |
Decreased neutrophils | 30 | 9 | 80 | 50 |
Previously Untreated Cisplatin-Ineligible Patients with Locally Advanced or mUC
EV-103
The safety of PADCEV was evaluated in combination with intravenous pembrolizumab in a multi cohort trial (EV-103) in 121 patients with locally advanced or mUC who were not eligible for cisplatin-containing chemotherapy and received at least one dose of PADCEV 1.25 mg/kg and pembrolizumab [see Clinical Studies (14 )] . The median duration of exposure to PADCEV was 7 months (range: 0.6 to 33 months).
Serious adverse reactions occurred in 50% of patients treated with PADCEV in combination with intravenous pembrolizumab. The most common serious adverse reactions (≥2%) were acute kidney injury (7%), urinary tract infection (7%), urosepsis (5%), sepsis (3.3%), pneumonia (3.3%), hematuria (3.3%), pneumonitis/ILD (3.3%), urinary retention (2.5%), diarrhea (2.5%), myasthenia gravis (2.5%), myositis (2.5%), anemia (2.5%), and hypotension (2.5%).
Fatal adverse reactions occurred in 5% of patients treated with PADCEV in combination with intravenous pembrolizumab including sepsis (1.6%), bullous dermatitis (0.8%), myasthenia gravis (0.8%), and pneumonitis/ILD (0.8%).
Adverse reactions leading to discontinuation of PADCEV occurred in 36% of patients. The most common adverse reactions (≥2%) leading to discontinuation of PADCEV were peripheral neuropathy (20%) and rash (6%).
Adverse reactions leading to dose interruption of PADCEV occurred in 69% of patients. The most common adverse reactions (≥2%) leading to dose interruption of PADCEV were peripheral neuropathy (18%), rash (12%), increased lipase (6%), pneumonitis/ILD (6%), diarrhea (4.1%), acute kidney injury (3.3%), increased alanine aminotransferase (3.3%), fatigue (3.3%), neutropenia (3.3%), urinary tract infection (3.3%), increased amylase (2.5%), anemia (2.5%), COVID-19 (2.5%), hyperglycemia (2.5%), and hypotension (2.5%).
Adverse reactions leading to dose reduction of PADCEV occurred in 45% of patients. The most common adverse reactions (≥2%) leading to dose reduction of PADCEV were peripheral neuropathy (17%), rash (12%), fatigue (5%), neutropenia (5%), and diarrhea (4.1%).
Table 9 summarizes the most common (≥20%) adverse reactions in EV-103.
| Adverse Reaction | PADCEV in combination with intravenous pembrolizumab n=121 | |
|---|---|---|
| All Grades % | Grade 3-4 % | |
Skin and subcutaneous tissue disorders | ||
Rash Includes: multiple terms. | 71 | 21 |
Alopecia | 52 | 0 |
Pruritus | 40 | 3.3 |
Dry skin | 21 | 0.8 |
Nervous system disorders | ||
Peripheral neuropathy | 65 | 3.3 |
Dysgeusia | 35 | 0 |
Dizziness | 23 | 0 |
General disorders and administration site conditions | ||
Fatigue | 60 | 11 |
Peripheral edema | 26 | 0 |
Investigations | ||
Decreased weight | 48 | 5 |
Gastrointestinal disorders | ||
Diarrhea | 45 | 7 |
Nausea | 36 | 0.8 |
Constipation | 27 | 0 |
Metabolism and nutrition disorders | ||
Decreased appetite | 38 | 0.8 |
Infections and infestations | ||
Urinary tract infection | 30 | 12 |
Eye disorders | ||
Dry eye | 25 | 0 |
Musculoskeletal and connective tissue disorders | ||
Arthralgia | 23 | 1.7 |
Clinically relevant adverse reactions (<20%) include vomiting (20%), pyrexia (18%), hypothyroidism (11%), pneumonitis/ILD (10%), skin hyperpigmentation (8%), myasthenia gravis (2.5%), myositis (3.3%), and infusion site extravasation (0.8%).
| Laboratory Abnormality | PADCEV in combination with intravenous pembrolizumab | |
|---|---|---|
| All Grades The denominator used to calculate the rate varied from 114 to 121 based on the number of patients with a baseline value and at least one post-treatment value. % | Grade 3-4 % | |
Chemistry | ||
Increased glucose | 74 | 13 |
Increased aspartate aminotransferase | 73 | 9 |
Increased creatinine | 69 | 3.3 |
Decreased sodium | 60 | 19 |
Increased alanine aminotransferase | 60 | 7 |
Increased lipase | 59 | 32 |
Decreased albumin | 59 | 4.2 |
Decreased phosphate | 51 | 15 |
Decreased potassium | 35 | 8 |
Increased potassium | 27 | 1.7 |
Increased calcium | 27 | 4.2 |
Hematology | ||
Decreased hemoglobin | 69 | 15 |
Decreased lymphocytes | 64 | 17 |
Decreased neutrophils | 32 | 12 |
Previously Treated Locally Advanced or mUC
EV-301
The safety of PADCEV was evaluated as a single agent in EV-301 in patients with locally advanced or mUC (n=296) who received at least one dose of PADCEV 1.25 mg/kg and who were previously treated with a PD-1 or PD-L1 inhibitor and a platinum-based chemotherapy [see Clinical Studies (14 )] . Routine ophthalmologic exams were not conducted in EV-301. The median duration of exposure to PADCEV was 5 months (range: 0.5 to 19 months).
Serious adverse reactions occurred in 47% of patients treated with PADCEV. The most common serious adverse reactions (≥2%) were urinary tract infection, acute kidney injury (7% each), and pneumonia (5%). Fatal adverse reactions occurred in 3% of patients, including multiorgan dysfunction (1%), hepatic dysfunction, septic shock, hyperglycemia, pneumonitis/ILD, and pelvic abscess (0.3% each).
Adverse reactions leading to discontinuation occurred in 17% of patients; the most common adverse reactions (≥2%) leading to discontinuation were peripheral neuropathy (5%) and rash (4%).
Adverse reactions leading to dose interruption occurred in 61% of patients; the most common adverse reactions (≥4%) leading to dose interruption were peripheral neuropathy (23%), rash (11%), and fatigue (9%).
Adverse reactions leading to dose reduction occurred in 34% of patients; the most common adverse reactions (≥2%) leading to dose reduction were peripheral neuropathy (10%), rash (8%), decreased appetite (3%), and fatigue (3%).
Table 11 summarizes the most common (≥15%) adverse reactions in EV-301.
| Adverse Reaction | PADCEV n=296 | Chemotherapy n=291 | ||
|---|---|---|---|---|
| All Grades % | Grade 3-4 % | All Grades % | Grade 3-4 % | |
Skin and subcutaneous tissue disorders | ||||
Rash Includes: multiple terms. | 54 | 14 | 20 | 0.3 |
Alopecia | 47 | 0 | 38 | 0 |
Pruritus | 34 | 2 | 7 | 0 |
Dry skin | 17 | 0 | 4 | 0 |
General disorders and administration site conditions | ||||
Fatigue | 50 | 9 | 40 | 7 |
Pyrexia | 22 | 2 | 14 | 0 |
Nervous system disorders | ||||
Peripheral neuropathy | 50 | 5 | 34 | 3 |
Dysgeusia | 26 | 0 | 8 | 0 |
Metabolism and nutrition disorders | ||||
Decreased appetite | 41 | 5 | 27 | 2 |
Gastrointestinal disorders | ||||
Diarrhea | 35 | 4 | 23 | 2 |
Nausea | 30 | 1 | 25 | 2 |
Constipation | 28 | 1 | 25 | 2 |
Abdominal Pain | 20 | 1 | 14 | 3 |
Musculoskeletal and connective tissue disorders | ||||
Musculoskeletal Pain | 25 | 2 | 35 | 5 |
Eye Disorders | ||||
Dry eye | 24 | 0.7 | 6 | 0.3 |
Infections and infestations | ||||
Urinary Tract Infection | 17 | 6 | 13 | 3 |
Vascular disorders | ||||
Hemorrhage | 17 | 3 | 13 | 2 |
Investigations | ||||
Decreased weight | 16 | 0.3 | 7 | 0 |
Clinically relevant adverse reactions (<15%) include vomiting (14%), increased aspartate aminotransferase (12%), hyperglycemia (10%), increased alanine aminotransferase (9%), skin hyperpigmentation (8%), pneumonitis/ILD (3%), and infusion site extravasation (0.7%).
| Laboratory Abnormality | PADCEV The denominator used to calculate the rate varied from 262 to 287 based on the number of patients with a baseline value and at least one post-treatment value. | Chemotherapy | ||
|---|---|---|---|---|
| Grades 2-4 % | Grade 3-4 % | Grades 2-4 % | Grade 3-4 % | |
Hematology | ||||
Decreased lymphocytes | 41 | 14 | 34 | 18 |
Decreased hemoglobin | 28 | 4 | 42 | 14 |
Decreased neutrophils | 27 | 12 | 25 | 17 |
Chemistry | ||||
Decreased phosphate | 39 | 8 | 24 | 6 |
Increased glucose (non-fasting) | 33 | 9 | 27 | 6 |
Increased creatinine | 18 | 2 | 13 | 0 |
Decreased potassium | 16 | 2 | 7 | 3 |
Increased lipase | 13 | 8 | 7 | 4 |
Decreased sodium | 8 | 8 | 5 | 5 |
EV-201, Cohort 1
The safety of PADCEV was evaluated as a single agent in EV-201, Cohort 1 in patients (n=125) with locally advanced or mUC who had received prior treatment with a PD-1 or PD-L1 inhibitor and platinum-based chemotherapy [see Clinical Studies (14 )]. Patients received PADCEV 1.25 mg/kg on Days 1, 8, and 15 of a 28-day cycle until disease progression or unacceptable toxicity. The median duration of exposure to PADCEV was 4.6 months (range: 0.5 to 15.6 months).
Serious adverse reactions occurred in 46% of patients treated with PADCEV. The most common serious adverse reactions (≥3%) were urinary tract infection (6%), cellulitis (5%), febrile neutropenia (4%), diarrhea (4%), sepsis (3%), acute kidney injury (3%), dyspnea (3%), and rash (3%). Fatal adverse reactions occurred in 3.2% of patients, including acute respiratory failure, aspiration pneumonia, cardiac disorder, sepsis, and pneumonitis/ILD (each 0.8%).
Adverse reactions leading to discontinuation occurred in 16% of patients; the most common adverse reaction leading to discontinuation was peripheral neuropathy (6%).
Adverse reactions leading to dose interruption occurred in 64% of patients; the most common adverse reactions leading to dose interruption were peripheral neuropathy (18%), rash (9%), and fatigue (6%).
Adverse reactions leading to dose reduction occurred in 34% of patients; the most common adverse reactions leading to dose reduction were peripheral neuropathy (12%), rash (6%), and fatigue (4%).
Table 13 summarizes the All Grades and Grades 3-4 adverse reactions reported in patients in EV-201, Cohort 1.
| Adverse Reaction | PADCEV n=125 | |
|---|---|---|
| All Grades % | Grade 3-4 % | |
General disorders and administration site conditions | ||
Fatigue Includes: multiple terms. | 56 | 6 |
Nervous system disorders | ||
Peripheral neuropathy | 56 | 4 |
Dysgeusia | 42 | 0 |
Metabolism and nutrition disorders | ||
Decreased appetite | 52 | 2 |
Skin and subcutaneous tissue disorders | ||
Rash | 52 | 13 |
Alopecia | 50 | 0 |
Dry skin | 26 | 0 |
Pruritus | 26 | 2 |
Gastrointestinal disorders | ||
Nausea | 45 | 3 |
Diarrhea | 42 | 6 |
Vomiting | 18 | 2 |
Eye disorders | ||
Dry eye | 40 | 0 |
Clinically relevant adverse reactions (<15%) include skin hyperpigmentation (14%), herpes zoster (3%), pneumonitis/ILD (2%), and infusion site extravasation (2%).
| Laboratory Abnormality | PADCEV | |
|---|---|---|
| Grades 2-4 Denominator for each laboratory parameter is based on the number of patients with a baseline and post-treatment laboratory value available for 121 or 122 patients. % | Grade 3-4 % | |
Hematology | ||
Decreased hemoglobin | 34 | 10 |
Decreased lymphocytes | 32 | 10 |
Decreased neutrophils | 14 | 5 |
Chemistry | ||
Decreased phosphate | 34 | 10 |
Increased glucose (non-fasting) | 27 | 8 |
Increased creatinine | 20 | 2 |
Decreased potassium | 19 Includes Grade 1 (potassium 3.0-3.5 mmol/L) – Grade 4. | 1 |
Increased lipase | 14 | 9 |
Decreased sodium | 8 | 8 |
Increased urate | 7 | 7 |
EV-201, Cohort 2
The safety of PADCEV was evaluated as a single agent in EV-201, Cohort 2 in patients with locally advanced or mUC (n=89) who received at least one dose of PADCEV 1.25 mg/kg and had prior treatment with a PD-1 or PD-L1 inhibitor and were not eligible for cisplatin-based chemotherapy. The median duration of exposure was 5.98 months (range: 0.3 to 24.6 months).
Serious adverse reactions occurred in 39% of patients treated with PADCEV. The most common serious adverse reactions (≥3%) were pneumonia, sepsis, and diarrhea (5% each). Fatal adverse reactions occurred in 8% of patients, including acute kidney injury (2.2%), metabolic acidosis, sepsis, multiorgan dysfunction, pneumonia, and pneumonitis/ILD (1.1% each).
Adverse reactions leading to discontinuation occurred in 20% of patients; the most common adverse reaction (≥2%) leading to discontinuation was peripheral neuropathy (7%).
Adverse reactions leading to dose interruption occurred in 60% of patients; the most common adverse reactions (≥3%) leading to dose interruption were peripheral neuropathy (19%), rash (9%), fatigue (8%), diarrhea (5%), increased aspartate aminotransferase (3%), and hyperglycemia (3%).
Adverse reactions leading to dose reduction occurred in 49% of patients; the most common adverse reactions (≥3%) leading to dose reduction were peripheral neuropathy (19%), rash (11%), and fatigue (7%).
Table 15 summarizes the All Grades and Grades 3-4 adverse reactions reported in patients in EV-201, Cohort 2.
| Adverse Reaction | PADCEV n=89 | |
|---|---|---|
| All Grades (%) | Grades 3-4 (%) | |
Skin and subcutaneous tissue disorders | ||
Rash Includes: multiple terms. | 66 | 17 |
Alopecia | 53 | 0 |
Pruritus | 35 | 3 |
Dry skin | 19 | 1 |
Nervous system disorders | ||
Peripheral neuropathy | 58 | 8 |
Dysgeusia | 29 | 0 |
General disorders and administration site conditions | ||
Fatigue | 48 | 11 |
Metabolism and nutrition disorders | ||
Decreased appetite | 40 | 6 |
Hyperglycemia | 16 | 9 |
Gastrointestinal disorders | ||
Diarrhea | 36 | 8 |
Nausea | 30 | 1 |
Investigations | ||
Decreased weight | 35 | 1 |
Eye disorders | ||
Dry eye | 30 | 0 |
Clinically relevant adverse reactions (<15%) include vomiting (13%), increased aspartate aminotransferase (12%), increased lipase (11%), increased alanine aminotransferase (10%), skin hyperpigmentation (4%), pneumonitis/ILD (4%), and infusion site extravasation (1%).
| Laboratory Abnormality | PADCEV n=88 Based on the number of patients with a baseline value and at least one post-treatment value. | |
|---|---|---|
| Grades 2-4 % | Grade 3-4 % | |
Hematology | ||
Decreased lymphocytes | 43 | 15 |
Decreased hemoglobin | 34 | 5 |
Decreased neutrophils | 20 | 9 |
Chemistry | ||
Increased glucose (non-fasting) | 36 | 13 |
Decreased phosphate | 25 | 7 |
Increased creatinine | 23 | 3 |
Increased lipase | 18 | 11 |
Increased urate | 9 | 9 |
Increased potassium | 8 | 6 |
Decreased sodium | 7 | 7 |
Post Marketing Experience
The following adverse reactions have been identified during post-approval use of PADCEV. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Skin and subcutaneous tissue disorders: Epidermal necrosis, Stevens-Johnson syndrome, and toxic epidermal necrolysis [see Warnings and Precautions (5.1 )] .
DRUG INTERACTIONS
Concomitant use of dual P-gp and strong CYP3A4 inhibitors with PADCEV may increase the exposure to monomethyl auristatin E (MMAE). (7.1 )
Effects of Other Drugs on PADCEV
Dual P-gp and Strong CYP3A4 Inhibitors
Concomitant use with dual P-gp and strong CYP3A4 inhibitors may increase unconjugated MMAE exposure [see Clinical Pharmacology (12.3 )] , which may increase the incidence or severity of PADCEV toxicities. Closely monitor patients for signs of toxicity when PADCEV is given concomitantly with dual P-gp and strong CYP3A4 inhibitors.
DESCRIPTION
Enfortumab vedotin-ejfv is a Nectin-4 directed antibody-drug conjugate (ADC) comprised of a fully human anti-Nectin-4 IgG1 kappa monoclonal antibody (AGS-22C3) conjugated to the small molecule microtubule disrupting agent, monomethyl auristatin E (MMAE) via a protease-cleavable maleimidocaproyl valine-citrulline (vc) linker (SGD-1006). Conjugation takes place on cysteine residues that comprise the interchain disulfide bonds of the antibody to yield a product with a drug-to-antibody ratio of approximately 3.8:1. The molecular weight is approximately 152 kDa.
Figure 1. Structural Formula

Approximately 4 molecules of MMAE are attached to each antibody molecule. Enfortumab vedotin-ejfv is produced by chemical conjugation of the antibody and small molecule components. The antibody is produced by mammalian (Chinese hamster ovary) cells and the small molecule components are produced by chemical synthesis.
PADCEV (enfortumab vedotin-ejfv) for injection is provided as a sterile, preservative-free, white to off-white lyophilized powder in single-dose vials for intravenous use. PADCEV is supplied as a 20 mg per vial and a 30 mg per vial and requires reconstitution with Sterile Water for Injection, USP, (2.3 mL and 3.3 mL, respectively) resulting in a clear to slightly opalescent, colorless to slightly yellow solution with a final concentration of 10 mg/mL [see Dosage and Administration (2.3 )]. After reconstitution, each vial allows the withdrawal of 2 mL (20 mg) and 3 mL (30 mg). Each mL of reconstituted solution contains 10 mg of enfortumab vedotin-ejfv, histidine (1.4 mg), histidine hydrochloride monohydrate (2.31 mg), polysorbate 20 (0.2 mg), and trehalose dihydrate (55 mg) with a pH of 6.0.
CLINICAL PHARMACOLOGY
Mechanism of Action
Enfortumab vedotin-ejfv is an ADC. The antibody is a human IgG1 kappa directed against Nectin-4, an adhesion protein located on the surface of cells. The small molecule, MMAE, is a microtubule-disrupting agent, attached to the antibody via a protease-cleavable linker. Nonclinical data suggest that the anticancer activity of enfortumab vedotin-ejfv is due to the binding of the ADC to Nectin-4-expressing cells, followed by internalization of the ADC-Nectin-4 complex, and the release of MMAE via proteolytic cleavage. Release of MMAE disrupts the microtubule network within the cell, subsequently inducing cell cycle arrest and apoptosis. The combination of enfortumab vedotin-ejfv with a PD-1 blocking antibody resulted in up-regulation of immune function and increased anti-tumor activity in syngeneic mouse tumor models expressing Nectin-4.
Pharmacodynamics
In an exposure-response analysis for safety, higher enfortumab vedotin-ejfv exposure was associated with higher incidence of some adverse reactions (e.g., Grade ≥2 peripheral neuropathy, Grade ≥3 hyperglycemia). The exposure‑response relationship for efficacy has not been fully characterized.
Cardiac Electrophysiology
At the recommended dose, PADCEV had no large QTc prolongation (>20 msec).
Pharmacokinetics
Enfortumab vedotin-ejfv (ADC) pharmacokinetics were characterized after single and multiple doses in patients with solid tumors.
The pharmacokinetics of the ADC and unconjugated MMAE were consistent when assessed following PADCEV administration as a single agent and in combination with intravenous pembrolizumab after 1 treatment cycle.
The exposure parameters of the ADC and unconjugated MMAE (the cytotoxic component of enfortumab vedotin-ejfv) are summarized in Table 17 below. Peak ADC concentrations were observed near the end of intravenous infusion while peak unconjugated MMAE concentrations were observed approximately 2 days after PADCEV dosing. Minimal accumulation of the ADC and unconjugated MMAE was observed following repeat administration of PADCEV in patients. Steady-state concentrations of the ADC were reached after 1 treatment cycle for the ADC as a single agent and in combination with intravenous pembrolizumab.
| C max = maximum concentration, AUC 0-28d = area under the concentration-time curve from time zero to 28 days, C trough,0-28d = pre-dose concentration on day 28. | ||
Parameter | ADC Mean (± SD) | Unconjugated MMAE Mean (± SD) |
C max | 28 (6.1) µg/mL | 5.5 (3.0) ng/mL |
AUC 0-28d | 110 (26) µg∙d/mL | 85 (50) ng∙d/mL |
C trough,0-28d | 0.31 (0.18) µg/mL | 0.81 (0.88) ng/mL |
Distribution
The estimated mean steady-state volume of distribution of the ADC was 12.8 L following administration of PADCEV. In vitro , plasma protein binding of unconjugated MMAE ranged from 68% to 82%.
Elimination
The ADC and unconjugated MMAE exhibited multi-exponential declines with an elimination half-life of 3.6 days and 2.6 days, respectively. The mean clearance (CL) of the ADC and unconjugated MMAE was 0.11 L/h and 2.11 L/h, respectively. Elimination of unconjugated MMAE appeared to be limited by its rate of release from the ADC.
Metabolism
Catabolism of the ADC has not been studied in humans; however, it is expected to undergo catabolism to small peptides, amino acids, unconjugated MMAE, and unconjugated MMAE-related catabolites. The ADC releases MMAE via proteolytic cleavage, and unconjugated MMAE is primarily metabolized by CYP3A4 in vitro .
Excretion
The excretion of the ADC is not fully characterized. Following a single-dose of another ADC that contains unconjugated MMAE, 17% of the total unconjugated MMAE administered was recovered in feces and 6% in urine over a 1-week period, primarily as unchanged form. A similar excretion profile of unconjugated MMAE is expected after PADCEV administration.
Specific Populations
No clinically significant differences in the pharmacokinetics of the ADC or unconjugated MMAE were identified based on age (24 to 90 years), sex, race (White, Asian, or Black), renal impairment, and mild hepatic impairment (total bilirubin of 1 to 1.5 × ULN and any AST, or total bilirubin ≤ULN and AST >ULN). The effect of end-stage renal disease with or without dialysis and moderate or severe hepatic impairment (total bilirubin >1.5 × ULN and any AST) on the pharmacokinetics of the ADC or unconjugated MMAE is unknown.
Drug Interaction Trials
No clinical trials evaluating the drug-drug interaction potential of the ADC have been conducted.
Physiologically Based Pharmacokinetic (PBPK) Modeling Predictions:
Dual P-gp and Strong CYP3A4 Inhibitor: Concomitant use of PADCEV with ketoconazole (a dual P-gp and strong CYP3A4 inhibitor) is predicted to increase unconjugated MMAE C max by 15% and AUC by 38%.
Dual P-gp and Strong CYP3A4 Inducer: Concomitant use of PADCEV with rifampin (a dual P-gp and strong CYP3A4 inducer) is predicted to decrease unconjugated MMAE C max by 28% and AUC by 53%.
Sensitive CYP3A Substrates: Concomitant use of PADCEV is predicted not to affect exposure to midazolam (a sensitive CYP3A substrate).
In Vitro Studies
Transporter Systems: MMAE is a substrate of P-glycoprotein (P-gp) and is not an inhibitor of P-gp.
Immunogenicity
The observed incidence of anti-drug antibody (ADA) is highly dependent on the sensitivity and specificity of the assay. Differences in assay methods preclude meaningful comparisons of the incidence of ADA in the studies described below with the incidence of ADA in other studies, including those of PADCEV or of other enfortumab vedotin products.
ADA was evaluated during the treatment periods (up to 5.5 years) in nine clinical studies of PADCEV as a single agent or in combination with intravenous pembrolizumab at the approved recommended dosages. Anti‑enfortumab vedotin-ejfv antibodies developed in:
- 3.7% (25/684) of patients who received PADCEV as a single agent.
- 1.3% (2/156) of patients who received PADCEV in combination with intravenous pembrolizumab for the treatment of MIBC.
- 7% (34/485) of patients who received PADCEV in combination with intravenous pembrolizumab for the treatment of locally advanced or mUC.
Because of the low occurrence of ADA, the effect of the ADA on the pharmacokinetics, pharmacodynamics, safety, and/or effectiveness of PADCEV is unknown.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies with enfortumab vedotin-ejfv or the small molecule cytotoxic agent (MMAE) have not been conducted.
MMAE was genotoxic in the rat bone marrow micronucleus study through an aneugenic mechanism. This effect is consistent with the pharmacological effect of MMAE as a microtubule-disrupting agent. MMAE was not mutagenic in the bacterial reverse mutation assay (Ames test) or the L5178Y mouse lymphoma forward mutation assay.
Fertility studies with enfortumab vedotin-ejfv or MMAE have not been conducted. However, results of repeat-dose toxicity studies indicate the potential for enfortumab vedotin-ejfv to impair female and male reproductive function and fertility.
In repeat-dose toxicology studies conducted in rats for up to 13 weeks, doses ≥2 mg/kg enfortumab vedotin-ejfv (at exposures similar to the exposures at the recommended human dose) resulted in decreases in testes and epididymis weights, seminiferous tubule degeneration, spermatid/spermatocyte depletion in the testes and cell debris, sperm granuloma, and hypospermia/abnormal spermatids in the epididymis. Findings in the testes and epididymis did not reverse by the end of the recovery period.
MMAE-containing ADCs have been associated with adverse ovarian effects when administered to sexually immature animals. Adverse effects included decrease in, or absence of, secondary and tertiary ovarian follicles after weekly administration to cynomolgus monkeys in studies of 4-week duration. These effects showed a trend towards recovery 6 weeks after the end of dosing; no changes were observed in primordial follicles.
CLINICAL STUDIES
Urothelial Cancer
Neoadjuvant and Adjuvant Treatment of Cisplatin-Ineligible Patients with MIBC
EV-303
The efficacy of PADCEV in combination with intravenous pembrolizumab as neoadjuvant treatment and then continued after RC as adjuvant treatment was evaluated in EV-303 (NCT03924895), an open-label, randomized, multicenter trial that enrolled patients with previously untreated MIBC with predominant urothelial carcinoma histology and who were candidates for radical cystectomy (RC) with pelvic lymph node dissection (PLND) but were ineligible for or refused cisplatin-based chemotherapy. The study excluded patients with primary non-bladder (i.e., ureter, urethral, or renal pelvis) cancer of the urothelium and those with active autoimmune disease that required systemic therapy within 2 years of treatment or a medical condition that required immunosuppression.
Randomization was stratified by tumor stage (T2N0 vs T3/T4aN0 vs T1-T4aN1), cisplatin-eligibility (cisplatin-ineligible vs cisplatin-eligible but declined), and geographic region (United States vs European Union vs Rest of World).
Patients were randomized 1:1 to receive:
- Neoadjuvant PADCEV 1.25 mg/kg as an intravenous infusion on Days 1 and 8 in combination with intravenous pembrolizumab 200 mg as an intravenous infusion on Day 1 of a 21-day cycle for 3 cycles prior to surgery, followed by adjuvant PADCEV for up to 6 cycles and intravenous pembrolizumab for up to 14 cycles (21 days per cycle) (n=170).
- Immediate RC and PLND alone (n=174).
Treatment continued until completion of the treatment, disease progression, not undergoing or refusal of RC and PLND, disease recurrence in the adjuvant phase, or unacceptable toxicity. Assessment of tumor status, including CT/MRI, was performed at baseline, within 5 weeks prior to RC and PLND, and at 6 weeks post-surgery. Following RC and PLND, assessment of tumor status, including cystoscopy and urine cytology for patients who did not undergo surgery, was performed every 12 weeks up to 2 years, and every 24 weeks thereafter.
The median age was 73 years (range: 46 to 87 years); 78% were male; 78% were White, 16% were Asian, 3.2% were multiple, 1.2% were Black or African American, 0.3% American Indian or Alaska Native, and race in 1.2% was missing; 91% were not Hispanic or Latino, 6% were Hispanic or Latino, and 2.9% were not reported. Patients had a baseline Eastern Cooperative Oncology Group (ECOG) performance status of 0 (57%), 1 (29%), or 2 (14%). Eighteen percent were T2N0, 77% T3/T4aN0, and 4.9% T1-T4aN1. Among the 281 patients who were ineligible for cisplatin, 72% had baseline creatinine clearance of 30-59 mL/min, 17% had ECOG PS of 2, 21% had Grade 2 or greater hearing loss, 3.9% had NYHA Class III heart failure, and 13% met more than one cisplatin-ineligibility criterion. Ninety-one percent of patients had pure urothelial carcinoma histology; 4.4% had urothelial carcinoma with squamous differentiation, 2.6% had urothelial carcinoma with glandular differentiation, and 2% had urothelial carcinoma with other variant histology.
In the overall population, 149 (88%) patients in the PADCEV in combination with intravenous pembrolizumab arm and 156 (90%) patients in the RC and PLND alone arm underwent RC and PLND.
The trial was not designed to isolate the effect of PADCEV in combination with intravenous pembrolizumab in each phase (neoadjuvant or adjuvant) of treatment.
The major efficacy outcome measure was event-free survival (EFS) as assessed by blinded independent central review (BICR). Overall survival (OS) and pathological complete response (pCR) rate as assessed by blinded independent pathology review were additional efficacy outcome measures.
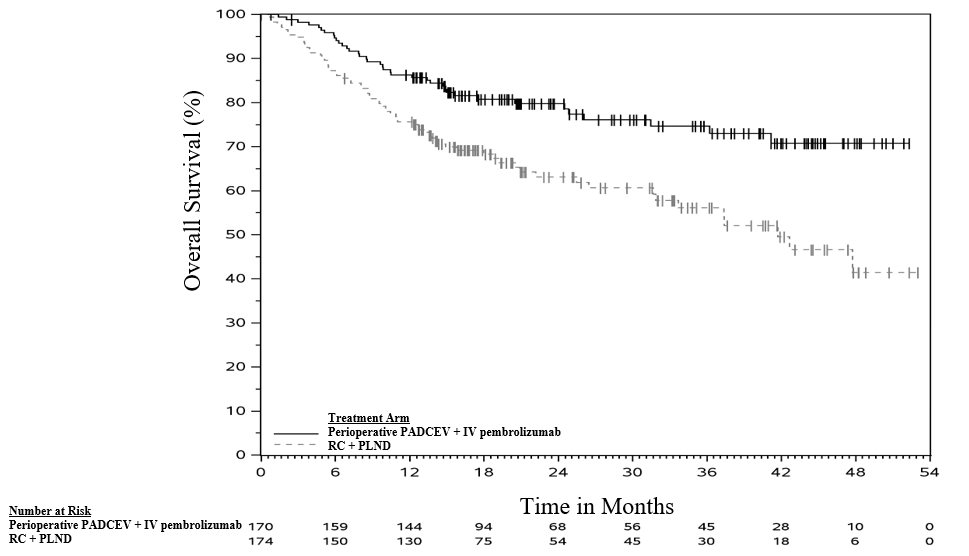
The trial demonstrated statistically significant improvements in EFS and OS in patients treated with neoadjuvant and adjuvant PADCEV in combination with intravenous pembrolizumab compared with RC and PLND alone.
Table 18 and Figures 2-3 summarize the efficacy results for EV-303.
| Endpoint | PADCEV with intravenous pembrolizumab before and after RC with PLND n=170 | RC with PLND alone n=174 |
|---|---|---|
| NR = Not Reached. | ||
Event-Free Survival EFS is defined as time from randomization to the first of: disease progression preventing curative surgery, failure to undergo surgery for participants with muscle invasive residual disease, incomplete surgical resection, local or distant recurrence after surgery, or death. | ||
Number (%) of patients with events | 48 (28) | 95 (55) |
Median in months Based on Kaplan-Meier estimates. (95% CI) | NR (37.3, NR) | 15.7 (10.3, 20.5) |
Hazard ratio Based on stratified Cox regression model. (95% CI) | 0.40 (0.28, 0.57) | |
p-value Based on stratified log-rank test. | <0.0001 | |
Overall Survival | ||
Number (%) of patients with events | 38 (22) | 68 (39) |
Median in months(95% CI) | NR (NR, NR) | 41.7 (31.8, NR) |
Hazard ratio(95% CI) | 0.50 (0.33, 0.74) | |
p-value | 0.0002 | |
Figure 2. Kaplan-Meier Plot of Event-Free Survival, EV-303
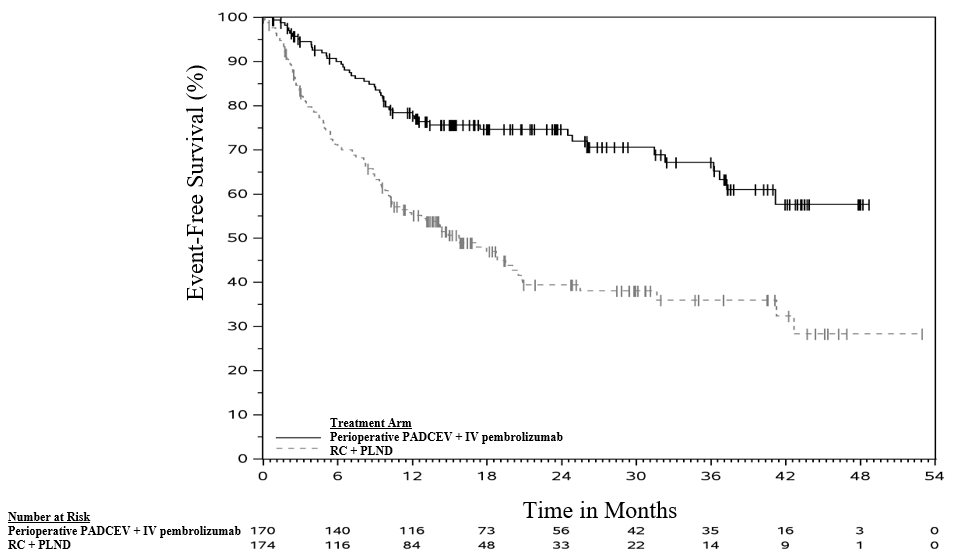
Figure 3. Kaplan-Meier Plot of Overall Survival, EV-303
The trial demonstrated a statistically significant difference in pCR rate (57.1% [95% CI: 49.3, 64.6] vs. 8.6% [95% CI: 4.9, 13.8]; p<0.0001).
Previously Untreated Locally Advanced or mUC
EV-302
The efficacy of PADCEV in combination with intravenous pembrolizumab was evaluated in EV-302 (NCT04223856), an open label, randomized, multicenter trial that enrolled 886 patients with locally advanced or mUC who received no prior systemic therapy for locally advanced or metastatic disease. Patients with active CNS metastases, ongoing sensory or motor neuropathy Grade ≥2, or uncontrolled diabetes defined as hemoglobin A1C (HbA1c) ≥8% or HbA1c ≥7% with associated diabetes symptoms were excluded.
Patients were randomized 1:1 to receive either:
- PADCEV 1.25 mg/kg on Days 1 and 8 of a 21-day cycle followed by intravenous pembrolizumab 200 mg on Day 1 of a 21‑day cycle. Treatment was continued until disease progression or unacceptable toxicity. In the absence of disease progression or unacceptable toxicity, pembrolizumab was continued for up to 2 years.
- Gemcitabine 1000 mg/m 2 on Days 1 and 8 of a 21-day cycle with cisplatin 70 mg/m 2 or carboplatin (AUC = 4.5 or 5) on Day 1 of a 21-day cycle. Treatment was continued until disease progression or unacceptable toxicity for up to 6 cycles.
Randomization was stratified by cisplatin eligibility, PD-L1 expression, and presence of liver metastases.
The median age was 69 years (range: 22 to 91 years); 77% were male; 67% were White, 22% were Asian, 1% were Black or African American, and 10% were unknown or other; 12% were Hispanic or Latino. Patients had a baseline Eastern Cooperative Oncology Group (ECOG) performance status of 0 (49%), 1 (47%), or 2 (3%). Forty-seven percent of patients had a documented baseline HbA1c of <5.7%. At baseline, 95% of patients had metastatic urothelial cancer, including 72% with visceral and 22% with liver metastases, and 5% had locally advanced urothelial cancer. Eighty-five percent of patients had urothelial carcinoma (UC) histology including 6% with UC mixed squamous differentiation and 2% with UC mixed other histologic variants. Forty-six percent of patients were considered cisplatin-ineligible and 54% were considered cisplatin-eligible at time of randomization.
The major efficacy outcome measures were overall survival (OS) and progression-free survival (PFS) as assessed by blinded independent central review (BICR) according to Response Evaluation Criteria in Solid Tumors (RECIST) v1.1. Additional efficacy outcome measures included objective response rate (ORR) as assessed by BICR.
The trial demonstrated statistically significant improvements in OS, PFS, and ORR for patients randomized to PADCEV in combination with intravenous pembrolizumab as compared to platinum-based chemotherapy. Efficacy results were consistent across all stratified patient subgroups. Table 19 and Figures 4-5 summarize the efficacy results for EV-302.
| Endpoint | PADCEV with intravenous pembrolizumab n=442 | Cisplatin or carboplatin with gemcitabine n=444 |
|---|---|---|
| NE = Not estimable. | ||
Overall Survival | ||
Number (%) of patients with events | 133 (30.1) | 226 (50.9) |
Median in months (95% CI) | 31.5 (25.4, NE) | 16.1 (13.9, 18.3) |
Hazard ratio (95% CI) Based on a stratified Cox proportional hazards model. | 0.47 (0.38, 0.58) | |
p-value Based on stratified log-rank test. , Two-sided p-value. | <0.0001 | |
Progression-Free Survival | ||
Number (%) of patients with events | 223 (50.5) | 307 (69.1) |
Median in months (95% CI) | 12.5 (10.4, 16.6) | 6.3 (6.2, 6.5) |
Hazard ratio (95% CI) | 0.45 (0.38, 0.54) | |
p-value , | <0.0001 | |
Confirmed Objective Response Rate Includes only patients with measurable disease at baseline (n=437 for PADCEV in combination with intravenous pembrolizumab, n=441 for chemotherapy). | ||
ORR (%) (95% CI) | 67.7 (63.1, 72.1) | 44.4 (39.7, 49.2) |
p-value , Cochran-Mantel-Haenszel test (CMH) controlling for stratification factors. | <0.0001 | |
Complete response rate (%) | 29.1 | 12.5 |
Partial response rate (%) | 38.7 | 32.0 |
Figure 4. Kaplan-Meier Plot of Overall Survival, EV-302

Figure 5. Kaplan-Meier Plot of Progression-Free Survival, EV-302

Cisplatin-Ineligible Patients with Previously Untreated Locally Advanced or mUC
EV-103
The efficacy of PADCEV in combination with intravenous pembrolizumab was evaluated in EV-103 (NCT03288545), an open-label, multi-cohort (dose escalation cohort, Cohort A, Cohort K) trial in patients with locally advanced or metastatic urothelial cancer who were ineligible for cisplatin-containing chemotherapy and received no prior systemic therapy for locally advanced or metastatic disease. Patients with active CNS metastases, ongoing sensory or motor neuropathy Grade ≥2, or uncontrolled diabetes defined as hemoglobin A1C (HbA1c) ≥8% or HbA1c ≥7% with associated diabetes symptoms were excluded from participating in the trial.
Patients in the dose escalation cohort (n=5), Cohort A (n=40), and Cohort K (n=76) received PADCEV 1.25 mg/kg as an IV infusion on Days 1 and 8 of a 21-day cycle followed by intravenous pembrolizumab 200 mg on Day 1 of a 21-day cycle. Patients were treated until disease progression or unacceptable toxicity.
A total of 121 patients received PADCEV in combination with intravenous pembrolizumab. The median age was 71 years (range: 51 to 91 years); 74% were male; 85% were White, 5% were Black, 4% were Asian, and 6% were other, unknown, or not reported. Ten percent of patients were Hispanic or Latino. Forty-five percent of patients had an ECOG performance status of 1 and 15% had an ECOG performance status of 2. Forty-seven percent of patients had a documented baseline HbA1c of <5.7%. Reasons for cisplatin ineligibility included: 60% with baseline creatinine clearance of 30-59 mL/min, 10% with ECOG PS of 2, 13% with Grade 2 or greater hearing loss, and 16% with more than one cisplatin-ineligibility criteria.
At baseline, 97.5% of patients had metastatic urothelial cancer and 2.5% of patients had locally advanced urothelial cancer. Thirty-seven percent of patients had upper tract disease. Eighty-four percent of patients had visceral metastasis at baseline including 22% with liver metastases. Thirty-nine percent of patients had transitional cell carcinoma (TCC) histology; 13% had TCC with squamous differentiation and 48% had TCC with other histologic variants.
The major efficacy outcome measures were ORR and DoR as assessed by BICR according to RECIST v1.1.
The median follow-up time for the dose escalation cohort + Cohort A was 44.7 months (range: 0.7 to 52.4 months) and for Cohort K was 14.8 months (range: 0.6 to 26.2 months).
Efficacy results are presented in Table 20 below.
| Endpoint | PADCEV in combination with intravenous pembrolizumab n=121 |
|---|---|
Confirmed ORR (95% CI) | 68% (58.7, 76.0) |
Complete response rate | 12% |
Partial response rate | 55% |
The median duration of response for the dose escalation cohort + Cohort A was 22.1 months (range: 1.0+ to 46.3+ months) and for Cohort K was not reached (range: 1.2 to 24.1+ months).
Previously Treated Locally Advanced or mUC
EV-301
The efficacy of PADCEV as a single agent was evaluated in EV-301 (NCT03474107), an open-label, randomized, multicenter trial that enrolled 608 patients with locally advanced or mUC who received prior treatment with a PD-1 or PD-L1 inhibitor and platinum-based chemotherapy. Patients were randomized 1:1 to receive either PADCEV 1.25 mg/kg on Days 1, 8, and 15 of a 28-day cycle or investigator’s choice of chemotherapy. Randomization was stratified by ECOG PS (0 vs 1), region of world (Western Europe vs US vs Rest of World), and presence of liver metastasis.
Patients were excluded if they had active central nervous system (CNS) metastases, ongoing sensory or motor neuropathy ≥ Grade 2, or uncontrolled diabetes defined as hemoglobin A1C (HbA1c) ≥8% or HbA1c ≥7% with associated diabetes symptoms.
The median age was 68 years (range: 30 to 88 years) and 77% were male. Racial demographics were reported as White (52%), Asian (33%), Black (0.7%), Native Hawaiian or Other Pacific Islander (0.2%), or not reported (15%). Nine percent of patients were Hispanic or Latino. All patients had a baseline ECOG performance status of 0 (40%) or 1 (60%). Thirty‑four percent of patients had tumors located in the upper tract that included the renal pelvis and ureter. Eighty percent of patients had visceral metastases including 31% with liver metastases. Seventy-six percent of patients had pure TCC histology; 14% had TCC with other histologic variants; and 10% had other tumor histologies including adenocarcinoma and squamous cell carcinoma. The median number of prior therapies was 2 (range 1 to ≥3). Sixty-three percent of patients received prior cisplatin-based regimens, 26% received prior carboplatin-based regimens, and an additional 11% received both cisplatin and carboplatin-based regimens. Patients on the control arm received docetaxel (38%), paclitaxel (36%), or vinflunine (25%).
The major efficacy outcome measures were OS, PFS, and ORR assessed by investigator using RECIST v1.1. Efficacy results were consistent across all stratified patient subgroups.
Table 21 and Figures 6-7 summarize the efficacy results for EV-301.
| Endpoint | PADCEV n=301 | Chemotherapy n=307 |
|---|---|---|
Overall Survival Based on log-rank test. Stratification factors were ECOG PS, region and liver metastasis. | ||
Number (%) of patients with events | 134 (44.5) | 167 (54.4) |
Median in months (95% CI) | 12.9 (10.6, 15.2) | 9.0 (8.1, 10.7) |
Hazard ratio (95% CI) | 0.70 (0.56, 0.89) | |
p-value | 0.0014 | |
Progression-Free Survival | ||
Number (%) of patients with events | 201 (66.8) | 231 (75.2) |
Median in months (95% CI) | 5.6 (5.3, 5.8) | 3.7 (3.5, 3.9) |
Hazard ratio (95% CI) | 0.62 (0.51, 0.75) | |
p-value | <0.0001 | |
Overall Response Rate (CR + PR) Based on Cochran-Mantel-Haenszel test. Stratification factors were ECOG PS, region and liver metastasis. | ||
ORR (%) (95% CI) | 40.6 (34.9, 46.5) | 17.9 (13.7, 22.8) |
p-value | <0.0001 | |
Complete response rate (%) | 4.9 | 2.7 |
Partial response rate (%) | 35.8 | 15.2 |
Figure 6. Kaplan-Meier Plot of Overall Survival, EV-301
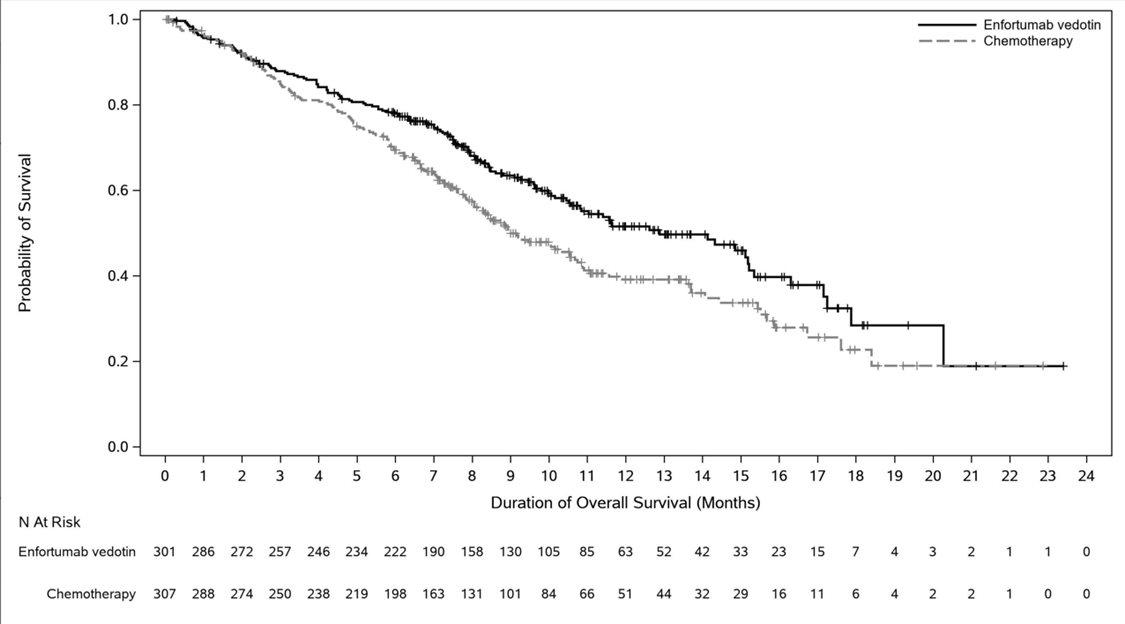
Figure 7. Kaplan-Meier Plot of Progression-Free Survival, EV-301
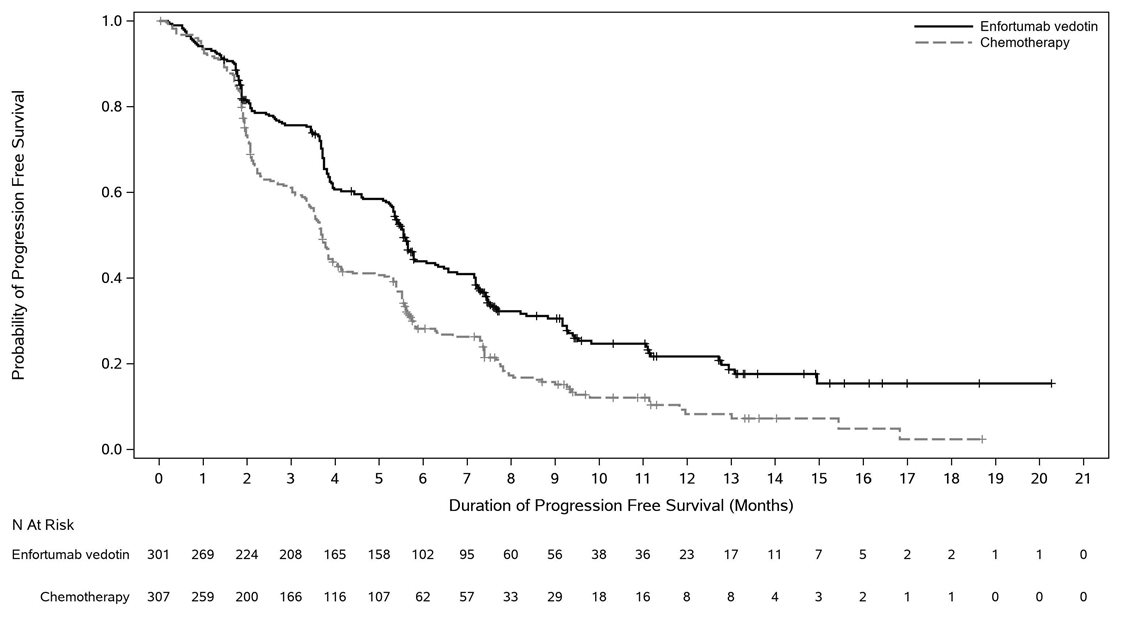
EV-201, Cohort 1
The efficacy of PADCEV as a single agent was also investigated in Cohort 1 of EV-201 (NCT03219333), a single-arm, multi-cohort, multicenter trial that enrolled 125 patients with locally advanced or mUC who received prior treatment with a PD-1 or PD-L1 inhibitor and a platinum-based chemotherapy. Patients were excluded if they had active central nervous system (CNS) metastases, ongoing sensory or motor neuropathy ≥ Grade 2, heart failure, or uncontrolled diabetes defined as hemoglobin A1C (HbA1c) ≥8% or HbA1c ≥7% with associated diabetes symptoms.
PADCEV was administered at a dose of 1.25 mg/kg, as an intravenous (IV) infusion on Days 1, 8, and 15 of each 28-day cycle.
The median age was 69 years (range: 40 to 84 years) and 70% were male. Racial demographics were reported as White (85%), Asian (9%), Black (2%), Other (0.8%), or not reported (4%). Four percent of patients were Hispanic or Latino. All patients had a baseline Eastern Cooperative Oncology Group (ECOG) performance status of 0 (32%) or 1 (68%). Ninety percent of patients had visceral metastases including 40% with liver metastases. Approximately two-thirds (67%) of patients had pure transitional cell carcinoma (TCC) histology; 33% had TCC with other histologic variants. The median number of prior systemic therapies was 3 (range: 1 to 6). Sixty-six percent of patients received prior cisplatin-based regimens, 26% received prior carboplatin-based regimens, and an additional 8% received both cisplatin and carboplatin‑based regimens.
The major efficacy outcome measures were confirmed objective response rate (ORR) and duration of response (DOR) assessed by BICR using RECIST v1.1.
Efficacy results are presented in Table 22 .
| Endpoint | PADCEV n=125 |
|---|---|
| NE = not estimable. | |
Confirmed ORR (95% CI) | 44% (35.1, 53.2) |
Complete Response Rate (CR) | 12% |
Partial Response Rate (PR) | 32% |
Median Based on patients (n=55) with a response by BICR. Duration of Response, months (95% CI) | 7.6 (6.3, NE) |
Previously Treated Cisplatin-Ineligible Patients with Locally Advanced or mUC
EV-201, Cohort 2
The efficacy of PADCEV as a single agent was also evaluated in Cohort 2 of EV-201, a single-arm, multi-cohort, multicenter trial in 89 patients with locally advanced or mUC who received prior treatment with a PD-1 or PD-L1 inhibitor and were cisplatin-ineligible and did not receive platinum in the locally advanced or metastatic setting. Patients were excluded if they had active CNS metastases, ongoing sensory or motor neuropathy ≥ Grade 2, heart failure, or uncontrolled diabetes defined as hemoglobin A1C (HbA1c) ≥8% or HbA1c ≥7% with associated diabetes symptoms.
PADCEV was administered at a dose of 1.25 mg/kg, as an intravenous (IV) infusion on Days 1, 8, and 15 of each 28-day cycle.
The median age was 75 years (range: 49 to 90 years), 74% were male. Racial demographics were reported as White (70%), Asian (22%), or not reported (8%). One percent of patients were Hispanic or Latino. Patients had a baseline ECOG performance status of 0 (42%), 1 (46%), and 2 (12%). Forty-three percent of patients had tumors located in the upper tract that included the renal pelvis and ureter. Seventy-nine percent of patients had visceral metastases and 24% had liver metastases.
Reasons for cisplatin ineligibility included: 66% with baseline creatinine clearance of 30-59 mL/min, 7% with ECOG PS of 2, 15% with Grade 2 or greater hearing loss, and 12% with more than one cisplatin-ineligibility criteria. Seventy percent of patients had TCC histology; 13% had TCC with squamous differentiation and 17% had TCC with other histologic variants.
The median number of prior systemic therapies was 1 (range: 1 to 4).
Efficacy results are presented in Table 23 below.
| NE = not estimable. | |
Endpoint | PADCEV n=89 |
Confirmed ORR (95% CI) | 51% (39.8, 61.3) |
Complete Response Rate (CR) | 22% |
Partial Response Rate (PR) | 28% |
Median Based on patients (n=45) with a response by BICR. Duration of Response, months (95% CI) | 13.8 (6.4, NE) |
HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
PADCEV (enfortumab vedotin-ejfv) 20 mg and 30 mg are supplied as a sterile, preservative-free, white to off-white lyophilized powder in single-dose vials. PADCEV vials are available in the following packages:
- Carton of one 20 mg single-dose vial (NDC 51144-020-01)
- Carton of one 30 mg single-dose vial (NDC 51144-030-01)
Storage
Store PADCEV vials refrigerated at 2ºC to 8ºC (36ºF to 46ºF) in the original carton. Do not freeze. Do not shake.
Special Handling
PADCEV is a hazardous drug. Follow applicable special handling and disposal procedures. 1
Mechanism of Action
Enfortumab vedotin-ejfv is an ADC. The antibody is a human IgG1 kappa directed against Nectin-4, an adhesion protein located on the surface of cells. The small molecule, MMAE, is a microtubule-disrupting agent, attached to the antibody via a protease-cleavable linker. Nonclinical data suggest that the anticancer activity of enfortumab vedotin-ejfv is due to the binding of the ADC to Nectin-4-expressing cells, followed by internalization of the ADC-Nectin-4 complex, and the release of MMAE via proteolytic cleavage. Release of MMAE disrupts the microtubule network within the cell, subsequently inducing cell cycle arrest and apoptosis. The combination of enfortumab vedotin-ejfv with a PD-1 blocking antibody resulted in up-regulation of immune function and increased anti-tumor activity in syngeneic mouse tumor models expressing Nectin-4.