Get your patient on Progesterone - Progesterone capsule (Progesterone)
Progesterone - Progesterone capsule prescribing information
WARNING: CARDIOVASCULAR DISORDERS, BREAST CANCER AND PROBABLE DEMENTIA FOR ESTROGEN PLUS PROGESTIN THERAPY
Cardiovascular Disorders and Probable Dementia
Estrogens plus progestin therapy should not be used for the prevention of cardiovascular disease or dementia. (See CLINICAL STUDIES and WARNINGS , Cardiovascular disorders and Probable dementia .)
The Women’s Health Initiative (WHI) estrogen plus progestin substudy reported increased risks of deep vein thrombosis, pulmonary embolism, stroke and myocardial infarction in postmenopausal women (50 to 79 years of age) during 5.6 years of treatment with daily oral conjugated estrogens (CE) [0.625 mg] combined with medroxyprogesterone acetate (MPA) [2.5 mg], relative to placebo. (See CLINICAL STUDIES and WARNINGS , Cardiovascular disorders .)
The WHI Memory Study (WHIMS) estrogen plus progestin ancillary study of the WHI reported an increased risk of developing probable dementia in postmenopausal women 65 years of age or older during 4 years of treatment with daily CE (0.625 mg) combined with MPA (2.5 mg), relative to placebo. It is unknown whether this finding applies to younger postmenopausal women. (See CLINICAL STUDIES and WARNINGS , Probable dementia and PRECAUTIONS , Geriatric Use .)
Breast Cancer
The WHI estrogen plus progestin substudy also demonstrated an increased risk of invasive breast cancer. (See CLINICAL STUDIES and WARNINGS , Malignant neoplasms , Breast Cancer .)
In the absence of comparable data, these risks should be assumed to be similar for other doses of CE and MPA, and other combinations and dosage forms of estrogens and progestins.
Progestins with estrogens should be prescribed at the lowest effective doses and for the shortest duration consistent with treatment goals and risks for the individual woman.
INDICATIONS AND USAGE
Progesterone capsules are indicated for use in the prevention of endometrial hyperplasia in nonhysterectomized postmenopausal women who are receiving conjugated estrogens tablets. They are also indicated for use in secondary amenorrhea.
DOSAGE AND ADMINISTRATION
Prevention of Endometrial Hyperplasia
Progesterone capsules should be given as a single daily dose at bedtime, 200 mg orally for 12 days sequentially per 28-day cycle, to a postmenopausal woman with a uterus who is receiving daily conjugated estrogens tablets.
Treatment of Secondary Amenorrhea
Progesterone capsules may be given as a single daily dose of 400 mg at bedtime for 10 days.
Some women may experience difficulty swallowing progesterone capsules. For these women, progesterone capsules should be taken with a glass of water while in the standing position.
CONTRAINDICATIONS
Progesterone capsules should not be used in women with any of the following conditions:
- Progesterone capsules should not be used in patients with known hypersensitivity to its ingredients. Progesterone capsules contain peanut oil and should never be used by patients allergic to peanuts.
- Undiagnosed abnormal genital bleeding.
- Known, suspected, or history of breast cancer.
- Active deep vein thrombosis, pulmonary embolism or history of these conditions.
- Active arterial thromboembolic disease (for example, stroke and myocardial infarction), or a history of these conditions.
- Known liver dysfunction or disease.
- Known or suspected pregnancy.
ADVERSE REACTIONS
See BOXED WARNING , WARNINGS and PRECAUTIONS . Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. In a multicenter, randomized, double-blind, placebo-controlled clinical trial, the effects of progesterone capsules on the endometrium was studied in a total of 875 postmenopausal women. Table 6 lists adverse reactions greater than or equal to 2 percent of women who received cyclic progesterone capsules 200 mg daily (12 days per calendar month cycle) with 0.625 mg conjugated estrogens or placebo.
| Progesterone Capsules 200 mg with Conjugated Estrogens 0.625 mg | Placebo | |
| (n=178) | (n=174) | |
| Headache | 31 | 27 |
| Breast Tenderness | 27 | 6 |
| Joint Pain | 20 | 29 |
| Depression | 19 | 12 |
| Dizziness | 15 | 9 |
| Abdominal Bloating | 12 | 5 |
| Hot Flashes | 11 | 35 |
| Urinary Problems | 11 | 9 |
| Abdominal Pain | 10 | 10 |
| Vaginal Discharge | 10 | 3 |
| Nausea / Vomiting | 8 | 7 |
| Worry | 8 | 4 |
| Chest Pain | 7 | 5 |
| Diarrhea | 7 | 4 |
| Night Sweats | 7 | 17 |
| Breast Pain | 6 | 2 |
| Swelling of Hands and Feet | 6 | 9 |
| Vaginal Dryness | 6 | 10 |
| Constipation | 3 | 2 |
| Breast Carcinoma | 2 | <1 |
| Breast Excisional Biopsy | 2 | <1 |
| Cholecystectomy | 2 | <1 |
Effects on Secondary Amenorrhea In a multicenter, randomized, double-blind, placebo-controlled clinical trial, the effects of progesterone capsules on secondary amenorrhea was studied in 49 estrogen-primed postmenopausal women. Table 7 lists adverse reactions greater than or equal to 5 percent of women who received progesterone capsules or placebo.
| Adverse Experience | Progesterone Capsules 400 mg | Placebo |
| n=25 | n=24 | |
| Percentage (%) of Patients | ||
| Fatigue | 8 | 4 |
| Headache | 16 | 8 |
| Dizziness | 24 | 4 |
| Abdominal Distention (Bloating) | 8 | 8 |
| Abdominal Pain (Cramping) | 20 | 13 |
| Diarrhea | 8 | 4 |
| Nausea | 8 | 0 |
| Back Pain | 8 | 8 |
| Musculoskeletal Pain | 12 | 4 |
| Irritability | 8 | 4 |
| Breast Pain | 16 | 8 |
| Infection Viral | 12 | 0 |
| Coughing | 8 | 0 |
In a multicenter, parallel-group, open label postmarketing dosing study consisting of three consecutive 28-day treatment cycles, 220 premenopausal women with secondary amenorrhea were randomized to receive daily conjugated estrogens therapy (0.625 mg conjugated estrogens) and progesterone capsules, 300 mg per day (n=113) or progesterone capsules, 400 mg per /day (n=107) for 10 days of each treatment cycle. Overall, the most frequently reported treatment-emergent adverse reactions, reported in greater than or equal to 5 percent of subjects, were nausea, fatigue, vaginal mycosis, nasopharyngitis, upper respiratory tract infection, headache, dizziness, breast tenderness, abdominal distension, acne, dysmenorrhea, mood swing, and urinary tract infection. Postmarketing Experience: The following additional adverse reactions have been reported with progesterone capsules. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate the frequency or establish a causal relationship to drug exposure. Genitourinary System: endometrial carcinoma, hypospadia, intra-uterine death, menorrhagia, menstrual disorder, metrorrhagia, ovarian cyst, spontaneous abortion. Cardiovascular: circulatory collapse, congenital heart disease (including ventricular septal defect and patent ductus arteriosus), hypertension, hypotension, tachycardia. Gastrointestinal: acute pancreatitis, cholestasis, cholestatic hepatitis, dysphagia, hepatic failure, hepatic necrosis, hepatitis, increased liver function tests (including alanine aminotransferase increased, aspartate aminotransferase increased, gamma-glutamyl transferase increased), jaundice, swollen tongue. Skin: alopecia, pruritus, urticaria. Eyes: blurred vision, diplopia, visual disturbance. Central Nervous System: aggression, convulsion, depersonalization, depressed consciousness, disorientation, dysarthria, loss of consciousness, paresthesia, sedation, stupor, syncope (with and without hypotension), transient ischemic attack, suicidal ideation. During initial therapy, a few women have experienced a constellation of many or all of the following symptoms: extreme dizziness and/or drowsiness, blurred vision, slurred speech, difficulty walking, loss of consciousness, vertigo, confusion, disorientation, feeling drunk, and shortness of breath. Miscellaneous: abnormal gait, anaphylactic reaction, arthralgia, blood glucose increased, choking, cleft lip, cleft palate, difficulty walking, dyspnea, face edema, feeling abnormal, feeling drunk, hypersensitivity, asthma, muscle cramp, throat tightness, tinnitus, vertigo, weight decreased, weight increased.
DESCRIPTION
Progesterone capsules contain micronized progesterone for oral administration. Progesterone has a molecular weight of 314.47 and a molecular formula of C 21 H 30 O 2 . Progesterone (pregn-4-ene-3, 20-dione) is a white or creamy white, crystalline powder or colorless crystals practically insoluble in water, soluble in alcohol, acetone and dioxane and sparingly soluble in vegetable oils, melting between 126º and 131ºC. The structural formula is: 
Progesterone is synthesized from a starting material from a plant source and is chemically identical to progesterone of human ovarian origin. Progesterone capsules are available in multiple strengths to afford dosage flexibility for optimum management. Progesterone capsules contain 100 mg or 200 mg micronized progesterone USP. The inactive ingredients for progesterone capsules include: gelatin, glycerin, hypromellose, iron oxide black, lecithin, peanut oil, propylene glycol, titanium dioxide.
CLINICAL PHARMACOLOGY
Progesterone capsules are an oral dosage form of micronized progesterone which is chemically identical to progesterone of ovarian origin. The oral bioavailability of progesterone is increased through micronization.
Pharmacokinetics
A. Absorption
After oral administration of progesterone as a micronized soft-gelatin capsule formulation, maximum serum concentrations were attained within 3 hours. The absolute bioavailability of micronized progesterone is not known. Table 1 summarizes the mean pharmacokinetic parameters in postmenopausal women after five oral daily doses of progesterone capsules 100 mg as a micronized soft-gelatin capsule formulation.
| 1. Mean ± S.D. | |||
| Parameter | Progesterone Capsules Daily Dose | ||
| 100 mg | 200 mg | 300 mg | |
| C max (ng/mL) | 17.3 ± 21.9 1 | 38.1 ± 37.8 | 60.6 ± 72.5 |
| T max (hr) | 1.5 ± 0.8 | 2.3 ± 1.4 | 1.7 ± 0.6 |
| AUC (0-10) (ng × hr/mL) | 43.3 ± 30.8 | 101.2 ± 66.0 | 175.7 ± 170.3 |
Serum progesterone concentrations appeared linear and dose proportional following multiple dose administration of progesterone capsules 100 mg over the dose range 100 mg per day to 300 mg per day in postmenopausal women. Although doses greater than 300 mg per day were not studied in females, serum concentrations from a study in male volunteers appeared linear and dose proportional between 100 mg per day and 400 mg per day. The pharmacokinetic parameters in male volunteers were generally consistent with those seen in postmenopausal women.
B. Distribution
Progesterone is approximately 96 percent to 99 percent bound to serum proteins, primarily to serum albumin (50 to 54 percent) and transcortin (43 to 48 percent).
C. Metabolism
Progesterone is metabolized primarily by the liver largely to pregnanediols and pregnanolones. Pregnanediols and pregnanolones are conjugated in the liver to glucuronide and sulfate metabolites. Progesterone metabolites which are excreted in the bile may be deconjugated and may be further metabolized in the intestine via reduction, dehydroxylation, and epimerization.
D. Excretion
The glucuronide and sulfate conjugates of pregnanediol and pregnanolone are excreted in the bile and urine. Progesterone metabolites are eliminated mainly by the kidneys. Progesterone metabolites which are excreted in the bile may undergo enterohepatic recycling or may be excreted in the feces.
E. Special Populations
The pharmacokinetics of progesterone capsules have not been assessed in low body weight or obese patients.
Hepatic Insufficiency: The effect of hepatic impairment on the pharmacokinetics of progesterone capsules has not been studied.
Renal Insufficiency: The effect of renal impairment on the pharmacokinetics of progesterone capsules has not been studied.
F. Food–Drug Interaction
Concomitant food ingestion increased the bioavailability of progesterone capsules relative to a fasting state when administered to postmenopausal women at a dose of 200 mg.
G. Drug Interactions
The metabolism of progesterone by human liver microsomes was inhibited by ketoconazole (IC 50 < 0.1 µM). Ketoconazole is a known inhibitor of cytochrome P450 3A4, hence these data suggest that ketoconazole or other known inhibitors of this enzyme may increase the bioavailability of progesterone. The clinical relevance of the in vitro findings is unknown. Coadministration of conjugated estrogens and progesterone capsules to 29 postmenopausal women over a 12-day period resulted in an increase in total estrone concentrations (C max 3.68 ng/mL to 4.93 ng/mL) and total equilin concentrations (C max 2.27 ng/mL to 3.22 ng/mL) and a decrease in circulating 17β estradiol concentrations (C max 0.037 ng/mL to 0.030 ng/mL). The half-life of the conjugated estrogens was similar with coadministration of progesterone capsules. Table 2 summarizes the pharmacokinetic parameters.
| 1. Total estrogens is the sum of conjugated and unconjugated estrogen. | ||||||
| Conjugated Estrogens | Conjugated Estrogens plus Progesterone Capsules | |||||
| Drug | C max (ng/mL) | T max (hr) | AUC (0-24h) (ng × h/mL) | C max (ng/mL) | T max (hr) | AUC (0-24h) (ng × h/mL) |
| Estradiol | 0.037 ± 0.048 | 12.7 ± 9.1 | 0.676 ± 0.737 | 0.030 ± 0.032 | 17.32 ± 1.21 | 0.561 ± 0.572 |
| Estrone Total 1 | 3.68 ± 1.55 | 10.6 ± 6.8 | 61.3 ± 26.36 | 4.93 ± 2.07 | 7.5 ± 3.8 | 85.9 ± 41.2 |
| Equilin Total 1 | 2.27 ± 0.95 | 6.0 ± 4.0 | 28.8 ± 13.0 | 3.22 ± 1.13 | 5.3 ± 2.6 | 38.1 ± 20.2 |
CLINICAL STUDIES
Effects on the endometrium
In a randomized, double-blind clinical trial, 358 postmenopausal women, each with an intact uterus, received treatment for up to 36 months. The treatment groups were: progesterone capsules at the dose of 200 mg per day for 12 days per 28-day cycle in combination with conjugated estrogens 0.625 mg per day (n=120); conjugated estrogens 0.625 mg per day only (n=119); or placebo (n=119). The subjects in all three treatment groups were primarily Caucasian women (87 percent or more of each group). The results for the incidence of endometrial hyperplasia in women receiving up to 3 years of treatment are shown in Table 3. A comparison of the progesterone capsules plus conjugated estrogens treatment group to the conjugated estrogens only group showed a significantly lower rate of hyperplasia (6 percent combination product versus 64 percent estrogen alone) in the progesterone capsules plus conjugated estrogens treatment group throughout 36 months of treatment.
| 1. Most advanced result to least advanced result: Adenocarcinoma > atypical hyperplasia > complex hyperplasia > simple hyperplasia | ||||||
| Endometrial Diagnosis | Treatment Group | |||||
| Conjugated Estrogens 0.625 mg + Progesterone Capsules 200 mg (cyclical) | Conjugated Estrogens 0.625 mg (alone) | Placebo | ||||
| Number of patients | % of patients | Number of patients | % of patients | Number of patients | % of patients | |
| n = 117 | n = 115 | n = 116 | ||||
| HYPERPLASIA 1 | 7 | 6 | 74 | 64 | 3 | 3 |
| Adenocarcinoma | 0 | 0 | 0 | 0 | 1 | 1 |
| Atypical hyperplasia | 1 | 1 | 14 | 12 | 0 | 0 |
| Complex hyperplasia | 0 | 0 | 27 | 23 | 1 | 1 |
| Simple hyperplasia | 6 | 5 | 33 | 29 | 1 | 1 |
The times to diagnosis of endometrial hyperplasia over 36 months of treatment are shown in Figure 1.
This figure illustrates graphically that the proportion of patients with hyperplasia was significantly greater for the conjugated estrogens group (64 percent) compared to the conjugated estrogens plus progesterone capsules group (6 percent). 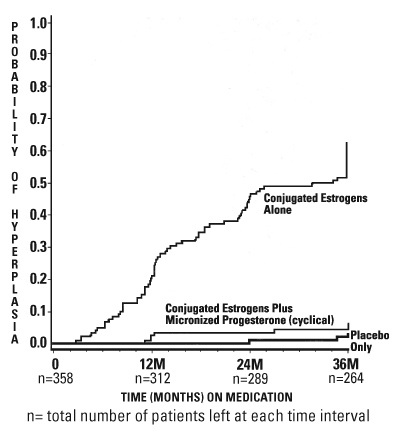
Figure 1. Time to Hyperplasia in Women Receiving up to 36 Months of Treatment
The discontinuation rates due to hyperplasia over the 36 months of treatment are as shown in Table 4. For any degree of hyperplasia, the discontinuation rate for patients who received conjugated estrogens plus progesterone capsules was similar to that of the placebo only group, while the discontinuation rate for patients who received conjugated estrogens alone was significantly higher. Women who permanently discontinued treatment due to hyperplasia were similar in demographics to the overall study population.
| Most Advanced Biopsy Result Through 36 Months of Treatment | Treatment Group | |||||
| Conjugated Estrogens + Progesterone Capsules (cyclical) | Conjugated Estrogens (alone) | Placebo | ||||
| n=120 | n=119 | n=119 | ||||
| Number of patients | % of patients | Number of patients | % of patients | Number of patients | % of patients | |
| Adenocarcinoma | 0 | 0 | 0 | 0 | 1 | 1 |
| Atypical hyperplasia | 1 | 1 | 10 | 8 | 0 | 0 |
| Complex hyperplasia | 0 | 0 | 21 | 18 | 1 | 1 |
| Simple hyperplasia | 1 | 1 | 13 | 11 | 0 | 0 |
Effects on secondary amenorrhea
In a single-center, randomized, double-blind clinical study that included premenopausal women with secondary amenorrhea for at least 90 days, administration of 10 days of progesterone capsules therapy resulted in 80 percent of women experiencing withdrawal bleeding within 7 days of the last dose of progesterone capsules, 300 mg per day (n=20), compared to 10 percent of women experiencing withdrawal bleeding in the placebo group (n=21). In a multicenter, parallel-group, open label, postmarketing dosing study that included premenopausal women with secondary amenorrhea for at least 90 days, administration of 10 days of progesterone capsules during two 28-day treatment cycles, 300 mg per day (n=107) or 400 mg per day (n=99), resulted in 73.8 percent and 76.8 percent of women, respectively, experiencing withdrawal bleeding. The rate of secretory transformation was evaluated in a multicenter, randomized, double-blind clinical study in estrogen-primed postmenopausal women. Progesterone capsules administered orally for 10 days at 400 mg per day (n=22) induced complete secretory changes in the endometrium in 45 percent of women compared to 0 percent in the placebo group (n=23). A second multicenter, parallel-group, open label postmarketing dosing study in premenopausal women with secondary amenorrhea for at least 90 days also evaluated the rate of secretory transformation. All subjects received daily oral conjugated estrogens over 3 consecutive 28-day treatment cycles and progesterone capsules, 300 mg per day (n=107) or 400 mg per day (n=99) for 10 days of each treatment cycle. The rate of complete secretory transformation was 21.5 percent and 28.3 percent, respectively.
Women’s Health Initiative Studies
The Women’s Health Initiative (WHI) enrolled approximately 27,000 predominantly healthy postmenopausal women in two substudies to assess the risks and benefits of daily oral conjugated estrogens (CE) [0.625 mg]-alone or in combination with medroxyprogesterone acetate (MPA) [2.5 mg] compared to placebo in the prevention of certain chronic diseases. The primary endpoint was the incidence of coronary heart disease [(CHD) defined as nonfatal myocardial infarction (MI), silent MI and CHD death], with invasive breast cancer as the primary adverse outcome. A “global index” included the earliest occurrence of CHD, invasive breast cancer, stroke, pulmonary embolism (PE), endometrial cancer (only in the CE plus MPA substudy), colorectal cancer, hip fracture, or death due to other cause. These sub studies did not evaluate the effects of CE-alone or CE plus MPA on menopausal symptoms.
WHI Estrogen Plus Progestin Substudy
The WHI estrogen plus progestin substudy was stopped early. According to the predefined stopping rule, after an average follow-up of 5.6 years of treatment, the increased risk of breast cancer and cardiovascular events exceeded the specified benefits included in the “global index.” The absolute excess risk of events in the “global index” was 19 per 10,000 women-years. For those outcomes included in the WHI “global index” that reached statistical significance after 5.6 years of follow-up, the absolute excess risks per 10,000 women-years in the group treated with CE plus MPA were 7 more CHD events, 8 more strokes, 10 more PEs, and 8 more invasive breast cancers, while the absolute risk reductions per 10,000 women-years were 6 fewer colorectal cancers and 5 fewer hip fractures. Results of the estrogen plus progestin substudy, which included 16,608 women (average 63 years of age, range 50 to 79; 83.9 percent White, 6.8 percent Black, 5.4 percent Hispanic, 3.9 percent Other) are presented in Table 5. These results reflect centrally adjudicated data after an average follow-up of 5.6 years.
| 1. Adapted from numerous WHI publications. WHI publications can be viewed at www.nhlbi.nih.gov/whi. 2. Results are based on centrally adjudicated data. 3. Nominal confidence intervals unadjusted for multiple looks and multiple comparisons. 4. Not included in Global Index. 5. Includes metastatic and non-metastatic breast cancer with the exception of in situ breast cancer. 6. All deaths, except from breast or colorectal cancer, definite or probable CHD, PE or cerebrovascular disease. 7. A subset of the events was combined in a “global index” defined as the earliest occurrence of CHD events, invasive breast cancer, stroke, pulmonary embolism, endometrial cancer, colorectal cancer, hip fracture, or death due to other causes. | |||
| Event | Relative Risk CE/MPA versus Placebo (95% nCI 3 ) | CE/MPA n = 8,506 | Placebo n = 8,102 |
| Absolute Risk per 10,000 Women-Years | |||
| CHD events | 1.23 (0.99 to 1.53) | 41 | 34 |
| Non-fatal MI | 1.28 (1.00 to 1.63) | 31 | 25 |
| CHD death | 1.10 (0.70 to 1.75) | 8 | 8 |
| All stroke | 1.31 (1.03 to 1.88) | 33 | 25 |
| Ischemic Stroke | 1.44 (1.09 to 1.90) | 26 | 18 |
| Deep vein thrombosis 4 | 1.95 (1.43 to 2.67) | 26 | 13 |
| Pulmonary embolism | 2.13 (1.45 to 3.11) | 18 | 8 |
| Invasive breast cancer 5 | 1.24 (1.01 to 1.54) | 41 | 33 |
| Colorectal cancer | 0.61 (0.42 to 0.87) | 10 | 16 |
| Endometrial cancer 4 | 0.81 (0.48 to 1.36) | 6 | 7 |
| Cervical cancer 4 | 1.44 (0.47 to 4.42) | 2 | 1 |
| Hip fracture | 0.67 (0.47 to 0.96) | 11 | 16 |
| Vertebral fractures 4 | 0.65 (0.46 to 0.92) | 11 | 17 |
| Lower arm/wrist fractures 4 | 0.71 (0.59 to 0.85) | 44 | 62 |
| Total fractures 4 | 0.76 (0.69 to 0.83) | 152 | 199 |
| Overall mortality 6 | 1.00 (0.83 to 1.19) | 52 | 52 |
| Global Index 7 | 1.13 (1.02 to 1.25) | 184 | 165 |
Timing of the initiation of estrogen plus progestin therapy relative to the start of menopause may affect the overall risk benefit profile. The WHI estrogen plus progestin substudy stratified for age showed in women 50 to 59 years of age a non-significant trend toward reducing risk of overall mortality [hazard ratio (HR) 0.69 (95 percent CI, 0.44 to 1.07)].
Women’s Health Initiative Memory Study
The estrogen plus progestin Women’s Health Initiative Memory Study (WHIMS), an ancillary study of WHI, enrolled 4,532 predominantly healthy postmenopausal women 65 years of age and older (47 percent were 65 to 69 years of age; 35 percent were 70 to 74 years of age; and 18 percent were 75 years of age and older) to evaluate the effects of daily CE (0.625 mg) plus MPA (2.5 mg) on the incidence of probable dementia (primary outcome) compared to placebo.
After an average follow-up of 4 years, the relative risk of probable dementia for CE plus MPA versus placebo was 2.05 (95 percent CI, 1.21 to 3.48). The absolute risk of probable dementia for CE plus MPA versus placebo was 45 versus 22 per 10,000 women-years. Probable dementia as defined in this study included Alzheimer’s disease (AD), vascular dementia (VaD) and mixed type (having features of both AD and VaD). The most common classification of probable dementia in the treatment group and the placebo group was AD. Since the ancillary study was conducted in women 65 to 79 years of age, it is unknown whether these findings apply to younger postmenopausal women. (See WARNINGS , Probable dementia and PRECAUTIONS , Geriatric Use. )
HOW SUPPLIED
Progesterone Capsules 100 mg are white to off white, round shaped soft gelatin capsules imprinted with “P1” using black ink and containing white to off white suspension.
Bottles of 100 NDC 59651-152-01
Progesterone Capsules 200 mg are white to off white, oval shaped soft gelatin capsules imprinted with “P2” using black ink and containing white to off white suspension.
Bottles of 100 NDC 59651-153-01
Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature].
Protect from excessive moisture. Dispense in tight, light-resistant container as defined in USP/NF, accompanied by a Patient Insert. Patient Information is available at: www.aurobindousa.com/product-medication-guides Keep out of reach of children. Distributed by: Aurobindo Pharma USA, Inc. 279 Princeton-Hightstown Road East Windsor, NJ 08520 Manufactured by: Eugia Pharma Specialities Limited Hyderabad – 500032 India