Triazolam - Triazolam tablet prescribing information
WARNING: RISKS FROM CONCOMITANT USE WITH OPIOIDS; ABUSE, MISUSE, AND ADDICTION; and DEPENDENCE AND WITHDRAWAL REACTIONS
- Concomitant use of benzodiazepines and opioids may result in profound sedation, respiratory depression, coma, and death. Reserve concomitant prescribing of these drugs in patients for whom alternative treatment options are inadequate. Limit dosages and durations to the minimum required. Follow patients for signs and symptoms of respiratory depression and sedation [see Warnings and Precautions (5.1) , Drug Interactions (7.1) ] .
- The use of benzodiazepines, including triazolam, exposes users to risks of abuse, misuse, and addiction, which can lead to overdose or death. Abuse and misuse of benzodiazepines commonly involve concomitant use of other medications, alcohol, and/or illicit substances, which is associated with an increased frequency of serious adverse outcomes. Before prescribing triazolam and throughout treatment, assess each patient's risk for abuse, misuse, and addiction [see Warnings and Precautions (5.2) ].
- The continued use of benzodiazepines, including triazolam, may lead to clinically significant physical dependence. The risks of dependence and withdrawal increase with longer treatment duration and higher daily dose. Abrupt discontinuation or rapid dosage reduction of triazolam after continued use may precipitate acute withdrawal reactions, which can be life-threatening. To reduce the risk of withdrawal reactions, use a gradual taper to discontinue triazolam or reduce the dosage [see Dosage and Administration (2.3) , Warnings and Precautions (5.3) ] .
Warnings and Precautions (5.10 ) | 2/2023 |
INDICATIONS AND USAGE
Triazolam is indicated for the short-term treatment of insomnia (generally 7 to 10 days) in adults.
DOSAGE AND ADMINISTRATION
Dosing Information
The recommended dosage is 0.25 mg once daily before bedtime. A dosage of 0.125 mg once daily may be sufficient for some patients (e.g., patients with low body weight). A dosage of 0.5 mg should be used only for patients who do not respond adequately to a trial of a lower dose. The maximum recommended dosage is 0.5 mg once daily.
Use the lowest effective dose for the patient as there are significant dose related adverse reactions.
Use of triazolam for more than 3 weeks requires evaluation of the patient for a primary psychiatric or medical condition [see Warnings and Precautions (5.4 , 5.6) ] .
Prescriptions for triazolam should be written for short-term use (7 to 10 days) and it should not be prescribed in quantities exceeding a 1-month supply.
Use in Geriatric Patients
In geriatric patients, the recommended dosage is 0.125 mg to 0.25 mg once daily. Initiate therapy at 0.125 mg once daily. The 0.25 mg dose should be used only for patients who do not respond to a trial of the lower dose. The maximum recommended dosage is 0.25 mg once daily. Elderly patients have an increased risk of dose related adverse reactions [see Use in Specific Populations (8.5) ] .
Discontinuation or Dosage Reduction of Triazolam
To reduce the risk of withdrawal reactions, use a gradual taper to discontinue triazolam or reduce the dosage. If a patient develops withdrawal reactions, consider pausing the taper or increasing the dosage to the previous tapered dosage level. Subsequently decrease the dosage more slowly [see Warnings and Precautions (5.3), Drug Abuse and Dependence (9.3) ] .
DOSAGE FORMS AND STRENGTHS
- Tablets: 0.125 mg white, imprinted with "G3717"
- Tablets: 0.25 mg powder blue, scored, imprinted with "G3718"
USE IN SPECIFIC POPULATIONS
Lactation : A lactating woman may pump and discard breast milk during treatment and for 28 hours after triazolam administration. (8.2 )
Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to psychiatric medications, including triazolam, during pregnancy. Healthcare providers are encouraged to register patients by calling the National Pregnancy Registry for Psychiatric Medications at 1-866-961-2388 or visiting online at https://womensmentalhealth.org/pregnancyregistry/ .
Risk Summary
Neonates born to mothers using benzodiazepines late in pregnancy have been reported to experience symptoms of sedation and/or neonatal withdrawal [see Warnings and Precautions (5.10) and Clinical Considerations ] . Available data from published observational studies of pregnant women exposed to benzodiazepines do not report a clear association with benzodiazepines and major birth defects ( see Data ).
The background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
Clinical Considerations
Fetal/Neonatal Adverse Reactions
Benzodiazepines cross the placenta and may produce respiratory depression, hypotonia, and sedation in neonates. Monitor neonates exposed to triazolam during pregnancy or labor for signs of sedation, respiratory depression, hypotonia, and feeding problems. Monitor neonates exposed to triazolam during pregnancy for signs of withdrawal. Manage these neonates accordingly [see Warnings and Precautions (5.10) ].
Data
Human Data
Published data from observational studies on the use of benzodiazepines during pregnancy do not report a clear association with benzodiazepines and major birth defects. Although early studies reported an increased risk of congenital malformations with diazepam and chlordiazepoxide, there was no consistent pattern noted. In addition, the majority of more recent case-control and cohort studies of benzodiazepine use during pregnancy, which were adjusted for confounding exposures to alcohol, tobacco and other medications, have not confirmed these findings.
Animal Data
Oral administration of triazolam to pregnant rats and rabbits during the period of organogenesis caused skeletal developmental changes (variations and malformations) at maternally toxic doses in rats and at doses in rats and rabbits which are approximately equal to or greater than 200 times the maximum recommended human dose (MRHD) of 0.5 mg/day based on mg/m 2 body surface area. Oral administration of triazolam to male and female rats before mating, and continuing during gestation and lactation did not result in embryotoxicity at doses up to approximately 100 times the MRHD based on mg/m 2 body surface area, but did cause an increase in the number of stillbirths and postnatal pup mortalities at doses greater than or equal to approximately 40 times the MRHD based mg/m 2 body surface area. 14 C-triazolam was administered orally to pregnant mice. Drug-related material appeared uniformly distributed in the fetus with 14 C concentrations approximately the same as in the brain of the mother.
Lactation
Risk Summary
There are reports of sedation, poor feeding and poor weight gain in infants exposed to benzodiazepines through breast milk. There are no data on the presence of triazolam in human milk or the effects on milk production. Triazolam and its metabolites are present in the milk of lactating rats ( see Data ). When a drug is present in animal milk, it is likely that the drug will be present in human milk.
The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for triazolam and any potential adverse effects on the breastfed infant from triazolam or from the underlying maternal condition.
Clinical Considerations
Infants exposed to triazolam through breast milk should be monitored for sedation, poor feeding and poor weight gain. A lactating woman may consider interrupting breastfeeding and pumping and discarding breast milk during treatment and for 28 hours (approximately 5 elimination half-lives) after triazolam administration in order to minimize drug exposure to a breast fed infant.
Data
Both triazolam and triazolam metabolites were detected in milk of rats. Lactating rats were orally administered 0.3 mg/kg 14 C-triazolam; drug and metabolite levels were determined in milk collected at 6 and 24 hours after administration.
Pediatric Use
Safety and effectiveness of triazolam have not been established in pediatric patients.
Geriatric Use
Elderly patients exhibit higher plasma triazolam concentrations due to reduced clearance as compared with younger subjects at the same dose. Because elderly patients are especially susceptible to dose related adverse reactions and to minimize oversedation, the smallest effective dose should be used [see Dosage and Administration (2.2) , Clinical Pharmacology (12.3) ] .
CONTRAINDICATIONS
Triazolam is contraindicated in:
- Patients with known hypersensitivity to triazolam, any of component of triazolam, or other benzodiazepines. Reactions consistent with angioedema (involving the tongue, glottis, or larynx), dyspnea, and throat closing have been reported and may be fatal.
- Concomitant administration of strong cytochrome P450 (CYP 3A) enzyme inhibitors (e.g., ketoconazole, itraconazole, nefazodone, lopinavir, ritonavir) [see Warnings and Precautions (5.8) , Drug Interactions (7.1) ].
WARNINGS AND PRECAUTIONS
- Persistent or Worsening Insomnia : Since sleep disturbances may be the presenting manifestation of a physical and/or psychiatric disorder, symptomatic treatment of insomnia should be initiated only after a careful evaluation of the patient. The failure of insomnia to remit after 7 to 10 days of treatment may indicate the presence of a primary psychiatric and/or medical illness that should be evaluated. (5.4 )
- "Sleep-driving" and Other Complex Behaviors : Complex behaviors such as "sleep-driving" have been reported. The use of alcohol and other central nervous system (CNS) depressants with sedative-hypnotics appears to increase the risk, as well as doses exceeding the maximum recommended dose. (5.5 )
- CNS Manifestations : An increase in daytime anxiety, abnormal thinking, and behavioral changes have been reported. Emergence of any new behavioral changes require careful and immediate evaluation. (5.6 )
- Effects on Driving and Operating Heavy Machinery : Patients receiving triazolam should be cautioned against driving or operating heavy machinery, as well as avoiding concomitant use with alcohol and other CNS depressant drugs. (5.7 )
- Patients with Depression : Caution should be exercised in patients with signs or symptoms of depression that could be intensified by hypnotic drugs. Prescribe the least number of tablets feasible to avoid intentional overdose. (5.9 )
- Neonatal Sedation and Withdrawal Syndrome : Triazolam use during pregnancy can result in neonatal sedation and/or neonatal withdrawal. (5.10 , 8.1 )
Risks From Concomitant Use With Opioids
Concomitant use of benzodiazepines, including triazolam, and opioids may result in profound sedation, respiratory depression, coma, and death. Because of these risks, reserve concomitant prescribing of these drugs in patients for whom alternative treatment options are inadequate.
Observational studies have demonstrated that concomitant use of opioid analgesics and benzodiazepines increases the risk of drug-related mortality compared to use of opioids alone. If a decision is made to prescribe triazolam concomitantly with opioids, prescribe the lowest effective dosages and minimum durations of concomitant use, and follow patients closely for signs and symptoms of respiratory depression and sedation. In patients already receiving an opioid analgesic, prescribe a lower initial dose of triazolam than indicated in the absence of an opioid and titrate based on clinical response. If an opioid is initiated in a patient already taking triazolam, prescribe a lower initial dose of the opioid and titrate based upon clinical response.
Advise both patients and caregivers about the risks of respiratory depression and sedation when triazolam is used with opioids. Advise patients not to drive or operate heavy machinery until the effects of concomitant use with the opioid have been determined [see Drug Interactions (7.1) ] .
Abuse, Misuse, and Addiction
The use of benzodiazepines, including triazolam, exposes users to the risks of abuse, misuse, and addiction, which can lead to overdose or death. Abuse and misuse of benzodiazepines often (but not always) involve the use of doses greater than the maximum recommended dosage and commonly involve concomitant use of other medications, alcohol, and/or illicit substances, which is associated with an increased frequency of serious adverse outcomes, including respiratory depression, overdose, or death [see Drug Abuse and Dependence (9.2) ] .
Before prescribing triazolam and throughout treatment, assess each patient's risk for abuse, misuse, and addiction (e.g., using a standardized screening tool). Use of triazolam, particularly in patients at elevated risk, necessitates counseling about the risks and proper use of triazolam along with monitoring for signs and symptoms of abuse, misuse, and addiction. Prescribe the lowest effective dosage; avoid or minimize concomitant use of CNS depressants and other substances associated with abuse, misuse, and addiction (e.g., opioid analgesics, stimulants); and advise patients on the proper disposal of unused drug. If a substance use disorder is suspected, evaluate the patient and institute (or refer them for) early treatment, as appropriate.
Dependence and Withdrawal Reactions
To reduce the risk of withdrawal reactions, use a gradual taper to discontinue triazolam or reduce the dosage (a patient-specific plan should be used to taper the dose) [see Dosage and Administration (2.3) ] .
Patients at an increased risk of withdrawal adverse reactions after benzodiazepine discontinuation or rapid dosage reduction include those who take higher dosages, and those who have had longer durations of use.
Acute Withdrawal Reactions
The continued use of benzodiazepines, including triazolam, may lead to clinically significant physical dependence. Abrupt discontinuation or rapid dosage reduction of triazolam after continued use, or administration of flumazenil (a benzodiazepine antagonist) may precipitate acute withdrawal reactions, which can be life-threatening (e.g., seizures) [see Drug Abuse and Dependence (9.3) ] .
Protracted Withdrawal Syndrome
In some cases, benzodiazepine users have developed a protracted withdrawal syndrome with withdrawal symptoms lasting weeks to more than 12 months [see Drug Abuse and Dependence (9.3) ] .
Persistent or Worsening Insomnia
Since sleep disturbances may be the presenting manifestation of a physical and/or psychiatric disorder, symptomatic treatment of insomnia should be initiated only after a careful evaluation of the patient. The failure of insomnia to remit after 7 to 10 days of treatment may indicate the presence of a primary psychiatric and/or medical illness that should be evaluated. Worsening of insomnia or the emergence of new thinking or behavior abnormalities may be the consequence of an unrecognized psychiatric or physical disorder. Such findings have emerged during the course of treatment with sedative-hypnotic drugs.
"Sleep-driving" and Other Complex Behaviors
Complex behaviors such as "sleep-driving" (i.e., driving while not fully awake after ingestion of a sedative-hypnotic, with amnesia for the event) have been reported with triazolam use. These events can occur in sedative-hypnotic-naïve as well as in sedative-hypnotic-experienced persons. Although behaviors such as sleep-driving may occur with sedative-hypnotics alone at recommended dosages, the use of alcohol and other central nervous system (CNS) depressants with sedative-hypnotics appears to increase the risk of such behaviors, as does the use of sedative-hypnotics at doses exceeding the maximum recommended dose. Due to the risk to the patient and the community, discontinuation of sedative-hypnotics should be strongly considered for patients who report a "sleep-driving" episode.
Other complex behaviors (e.g., preparing and eating food, making phone calls, or having sex) have been reported in patients who are not fully awake after taking a sedative-hypnotic, including triazolam. As with sleep-driving, patients usually do not remember these events.
Central Nervous System Manifestations
An increase in daytime anxiety has been reported for triazolam after as few as 10 days of continuous use. In some patients this may be a manifestation of interdose withdrawal. If increased daytime anxiety is observed during treatment, discontinuation of treatment may be advisable.
A variety of abnormal thinking and behavior changes have been reported to occur in association with the use of benzodiazepine hypnotics including triazolam. Some of these changes may be characterized by decreased inhibition, e.g., aggressiveness and extroversion that seem excessive, similar to that seen with alcohol and other CNS depressants (e.g., sedative/hypnotics). Other kinds of behavioral changes have also been reported, for example, bizarre behavior, agitation, hallucinations, depersonalization. In primarily depressed patients, the worsening of depression, including suicidal thinking, has been reported in association with the use of benzodiazepines [see Warnings and Precautions (5.9) ] .
Some adverse reactions reported in association with the use of triazolam such as drowsiness, dizziness, light-headedness, and amnesia appear to be dose related. More serious behavioral phenomena such as confusion, bizarre or abnormal behavior, agitation, and hallucinations may also be dose related, but this evidence is inconclusive. Therapy should be initiated at the lowest effective dose [see Dosage and Administration (2.1) ] .
It can rarely be determined with certainty whether a particular instance of the abnormal behaviors listed above is drug induced, spontaneous in origin, or a result of an underlying psychiatric or physical disorder. Nonetheless, the emergence of any new behavioral sign or symptom of concern requires careful and immediate evaluation.
Anterograde amnesia of varying severity and paradoxical reactions have been reported following recommended dosages of triazolam. Data from several sources suggest that anterograde amnesia may occur at a higher rate with triazolam than with other benzodiazepine hypnotics. Because triazolam can cause drowsiness and a decreased level of consciousness, patients, particularly the elderly, are at higher risk of falls.
Cases of "traveler's amnesia" have been reported by individuals who have taken triazolam to induce sleep while traveling, such as during an airplane flight. In some of these cases, insufficient time was allowed for the sleep period prior to awakening and before beginning activity. Also, the concomitant use of alcohol may have been a factor in some cases.
Effects on Driving and Operating Heavy Machinery
Due to its depressant CNS effects, patients receiving triazolam should be cautioned against engaging in hazardous occupations requiring complete mental alertness such as operating machinery or driving a motor vehicle. For the same reason, patients should be cautioned about the concomitant use of alcohol and other CNS depressant drugs during treatment with triazolam.
Triazolam Interaction With Drugs That Inhibit Metabolism via Cytochrome P450 3A
The initial step in triazolam metabolism is hydroxylation catalyzed by CYP 3A. Drugs that inhibit this metabolic pathway may have a profound effect on the clearance of triazolam.
Strong CYP 3A Inhibitors
Triazolam is contraindicated in patients receiving strong inhibitors of CYP 3A such as ketoconazole, itraconazole, nefazodone, ritonavir, indinavir, nelfinavir, saquinavir, and lopinavir [see Contraindications (4) , Drug Interactions (7.1) ] .
Moderate and Weak CYP 3A Inhibitors
Triazolam should be used with caution in patients receiving moderate or weak inhibitors of CYP 3A. If coadministered, consider dose reduction of triazolam.
Macrolide Antibiotics
Coadministration of erythromycin increased the maximum plasma concentration, decreased clearance and increased half-life of triazolam [see Drug Interactions (7.1) , Clinical Pharmacology (12.3) ] ; caution and consideration of appropriate triazolam dose reduction are recommended. Similar caution should be observed during coadministration with clarithromycin and other macrolide antibiotics.
Cimetidine
Coadministration of cimetidine increased the maximum plasma concentration, decreased clearance and increased half-life of triazolam [see Drug Interactions (7.1) , Clinical Pharmacology (12.3) ] ; caution and consideration of appropriate triazolam dose reduction are recommended.
Patients With Depression
Benzodiazepines may worsen depression. Consequently, appropriate precautions (e.g., limiting the total prescription size and increased monitoring for suicidal ideation) should be considered in patients with depression .
Neonatal Sedation and Withdrawal Syndrome
Use of triazolam late in pregnancy can result in sedation (respiratory depression, lethargy, hypotonia) and /or withdrawal symptoms (hyperreflexia, irritability, restlessness, tremors, inconsolable crying, and feeding difficulties) in the neonate [see Use in Specific Populations (8.1) ] . Monitor neonates exposed to triazolam during pregnancy or labor for signs of sedation and monitor neonates exposed to triazolam during pregnancy for signs of withdrawal; manage these neonates accordingly.
Compromised Respiratory Function
In patients with compromised respiratory function, respiratory depression and apnea have been reported. Closely monitor patients with compromised respiratory function. If signs and symptoms of respiratory depression or apnea occur, consider discontinuation.
ADVERSE REACTIONS
The following serious adverse reactions are discussed in greater detail in other sections:
- Risks from Concomitant Use with Opioids [see Warnings and Precautions (5.1) ]
- Abuse, Misuse, and Addiction [see Warnings and Precautions (5.2) ]
- Dependence and Withdrawal Reactions [see Warnings and Precautions (5.3) ]
- Persistent or Worsening Insomnia [see Warnings and Precautions (5.4) ]
- "Sleep-driving" and Other Complex Behaviors [see Warnings and Precautions (5.5) ]
- Central Nervous System Manifestations [see Warnings and Precautions (5.6) ]
- Effects on Driving and Operating Heavy Machinery [see Warnings and Precautions (5.7) ]
- Patients with Depression [see Warnings and Precautions (5.9) ]
- Neonatal Sedation and Withdrawal Syndrome [see Warnings and Precautions (5.10) ]
- Compromised Respiratory Function [see Warnings and Precautions (5.11) ]
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The incidences cited below are estimates of clinical reactions among 1003 subjects who participated in the short term (duration of 1 to 42 days) placebo-controlled clinical trials of triazolam.
Adverse reactions leading to discontinuation in two multi-dose placebo controlled clinical trials include coordination disorders, drowsiness, grogginess, somnolence, depression, restlessness, dizziness, lightheadedness, headache, nausea, visual disturbance, nervousness, abdominal distress, bladder trouble, aching limbs, backache, and blepharitis.
| Event | Triazolam (N=1003) % Patients Reporting | Placebo (N=997) % Patients Reporting |
|---|---|---|
Central Nervous System | ||
Drowsiness | 14.0 | 6.4 |
Headache | 9.7 | 8.4 |
Dizziness | 7.8 | 3.1 |
Nervousness | 5.2 | 4.5 |
Light-headedness | 4.9 | 0.9 |
Coordination disorders/ataxia | 4.6 | 0.8 |
Gastrointestinal | ||
Nausea/vomiting | 4.6 | 3.7 |
In addition to the common reactions enumerated above in Table1, the following adverse reactions have been reported at an incidence of 0.9% to 0.5%: euphoria, tachycardia, tiredness, confusional states/memory impairment, cramps/pain, depression, and visual disturbances.
Adverse reactions reported at an incidence less than 0.5% include: constipation, taste alterations, diarrhea, dry mouth, dermatitis/allergy, dreaming/nightmares, insomnia, paresthesia, tinnitus, dysesthesia, weakness, congestion, and death from hepatic failure in a patient also receiving diuretic drugs.
Postmarketing Experience
The following adverse reactions have been identified during post-approval use of triazolam. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
General disorders and administration site conditions: Paradoxical drug reaction, chest pain and fatigue Gastrointestinal disorders: Tongue discomfort, glossitis, stomatitis Hepatobiliary disorders: Jaundice Injury, poisoning and procedural complications: Fall Metabolism and nutrition disorders: Anorexia Nervous system disorders : Anterograde amnesia, altered state of consciousness, dystonia, sedation, syncope, dysarthria and muscle spasticity Psychiatric disorders: Confusional state (disorientation, derealisation, depersonalization), mania, agitation, restlessness, irritability, sleep disorder and libido disorder, hallucination, delusion, aggression, somnambulism, and abnormal behavior Renal and urinary disorders: Urinary retention and urinary incontinence Reproductive system and breast disorders: Menstruation irregular Skin and subcutaneous tissue disorders: Pruritis
DRUG INTERACTIONS
Drugs Having Clinically Important Interactions With Triazolam
Table 2 includes clinically significant drug interactions with triazolam [see Clinical Pharmacology (12.3) ] .
Opioids | |
Clinical implication | The concomitant use of benzodiazepines and opioids increases the risk of respiratory depression because of actions at different receptor sites in the CNS that control respiration. Benzodiazepines interact at GABA A sites and opioids interact primarily at mu receptors. When benzodiazepines and opioids are combined, the potential for benzodiazepines to significantly worsen opioid-related respiratory depression exists. |
Prevention or management | Limit dosage and duration of concomitant use of triazolam and opioids, and monitor patients closely for respiratory depression and sedation [see Warnings and Precautions (5.1) ] . |
CNS Depressants | |
Clinical implication | Triazolam produces additive CNS depressant effects when co-administered with other CNS depressants. |
Prevention or management | Limit dosage and duration of triazolam during concomitant use with CNS depressants. |
Strong Inhibitors of CYP 3A | |
Clinical implication | Concomitant use of triazolam with strong CYP3A inhibitors has a profound effect on the clearance of triazolam, resulting in increased concentrations of triazolam and increased risk of adverse reactions [see Clinical Pharmacology (12.3) ]. |
Prevention or management | Do not administer triazolam with a strong CYP3A4 inhibitor [see Contraindications (4) , Warnings and Precautions (5.8) ]. |
Moderate and Weak Inhibitors of CYP 3A | |
Clinical implication | Concomitant use of triazolam with moderate or weak inhibitors of CYP3A inhibitors may increase the concentrations of triazolam, resulting in increased risk of adverse reactions [see Clinical Pharmacology (12.3) ]. |
Prevention or management | Use with caution and consider appropriate dose reduction of triazolam when coadministered with moderate and weak CYP3A inhibitors [see Warnings and Precautions (5.8) ]. |
Strong Inducers of CYP 3A | |
Clinical implication | Coadministration of triazolam with strong inducers of CYP3A4 can significantly decrease the plasma concentration of triazolam and may decrease effectiveness of triazolam. |
Prevention or management | Caution is recommended during coadministration of triazolam with strong inducers of CYP3A4. |
Interactions Based on Experience with Other Benzodiazepines or in vitro Studies with Triazolam | |
Clinical implication | Available data from clinical studies of benzodiazepines other than triazolam, from in vitro studies with triazolam, or from in vitro studies with benzodiazepines other than triazolam suggest a possible drug interaction with triazolam [see Clinical Pharmacology (12.3) ]. |
Prevention or management | Caution is recommended during coadministration of triazolam with any of these drugs. [see Warnings and Precautions (5.8) ]. |
DESCRIPTION
Triazolam is a triazolobenzodiazepine.
Triazolam is a white crystalline powder, soluble in alcohol and poorly soluble in water. It has a molecular weight of 343.21.
The chemical name for triazolam is 8-chloro-6-(o-chlorophenyl)-1-methyl-4H-s-triazolo-[4,3-α] [1,4] benzodiazepine.
The structural formula is represented below:
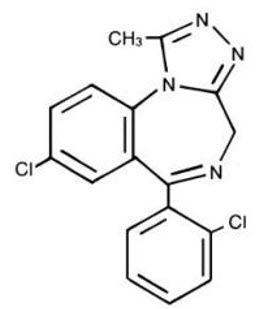
Each triazolam tablet, for oral administration, contains 0.125 mg or 0.25 mg of triazolam.
Inactive ingredients: 0.125 mg—cellulose, corn starch, docusate sodium, lactose, magnesium stearate, silicon dioxide, sodium benzoate; 0.25 mg—cellulose, corn starch, docusate sodium, FD&C Blue No. 2, lactose, magnesium stearate, silicon dioxide, sodium benzoate.
CLINICAL PHARMACOLOGY
Mechanism of Action
Triazolam is a benzodiazepine. Triazolam exerts its effect for the short-term treatment of insomnia through binding to the benzodiazepine site of the gamma-aminobutyric acid-A (GABA A ) receptors in the brain and enhances GABA-mediated synaptic inhibition.
Pharmacokinetics
Absorption
Peak plasma levels of triazolam are reached within 2 hours following oral administration. Following recommended doses of triazolam, triazolam peak plasma levels in the range of 1 to 6 ng/mL are seen. The plasma levels achieved are proportional to the dose given. In normal subjects treated for 7 days with four times the recommended dosage, there was no evidence of altered systemic bioavailability, rate of elimination, or accumulation.
Distribution
Extremely high concentrations of triazolam do not displace bilirubin bound to human serum albumin in vitro.
Elimination
Triazolam has a mean plasma elimination half-life in the range of 1.5 to 5.5 hours.
Metabolism
The initial step in triazolam metabolism is cytochrome P450 3A (CYP 3A)-mediated hydroxylation to form 1-hydroxytriazolam and 4-hydroxytriazolam, which are subsequently conjugated to form glucuronides.
Excretion
Triazolam and its metabolites, principally as conjugated glucuronides which are presumably inactive, are excreted primarily in the urine. Only small amounts of unmetabolized triazolam appear in the urine. The two primary metabolites accounted for 79.9% of urinary excretion. Urinary excretion appeared to be biphasic in its time course.
Specific Populations
Geriatric Patients
In a study of elderly (62 to 83 years old) versus younger subjects (21 to 41 years old) who received triazolam at the same dose levels (0.125 mg and 0.25 mg), the elderly experienced both greater sedation and impairment of psychomotor performance. These effects resulted largely from higher plasma concentrations of triazolam in the elderly.
Drug Interaction Studies
The effect of other drugs on triazolam:
Macrolide Antibiotics
Coadministration of erythromycin increased the maximum plasma concentration of triazolam by 46%, decreased clearance by 53%, and increased half-life by 35%.
Cimetidine
Coadministration of cimetidine increased the maximum plasma concentration of triazolam by 51%, decreased clearance by 55%, and increased half-life by 68%.
Isoniazid
Coadministration of isoniazid increased the maximum plasma concentration of triazolam by 20%, decreased clearance by 42%, and increased half-life by 31%.
Oral Contraceptives
Coadministration of oral contraceptives increased maximum plasma concentration by 6%, decreased clearance by 32%, and increased half-life by 16%.
Grapefruit Juice
Coadministration of grapefruit juice increased the maximum plasma concentration of triazolam by 25%, increased the area under the concentration curve by 48%, and increased half-life by 18%.
Ranitidine
Coadministration of ranitidine increased the maximum plasma concentration of triazolam by 30%, increased the area under the concentration curve by 27%, and increased half-life by 3.3%. Caution is recommended during coadministration with triazolam. Available data from clinical studies of benzodiazepines other than triazolam suggest a possible drug interaction with triazolam for the following: fluvoxamine, diltiazem, and verapamil. Data from in vitro studies of triazolam suggest a possible drug interaction with triazolam for the following: sertraline and paroxetine. Data from in vitro studies of benzodiazepines other than triazolam suggest a possible drug interaction with triazolam for the following: ergotamine, cyclosporine, amiodarone, nicardipine, and nifedipine.
The effect of triazolam on other drugs:
Warfarin
Triazolam Tablets 0.5 mg, in two separate studies, did not affect the prothrombin times or plasma warfarin levels in male volunteers administered sodium warfarin orally.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
No evidence of carcinogenic potential was observed in rats or mice administered triazolam in the diet for 24-months at doses greater than or equal to 900 times the MRHD of 0.5 mg, based on mg/m 2 body surface area.
Mutagenesis
Triazolam was not mutagenic in the in vitro Ames bacterial reverse mutation assay, and no DNA damage was observed in an in vitro alkaline elution assay in Chinese hamster lung fibroblast cells.
Impairment of Fertility
Female rats were administered triazolam in the diet for 14 days before cohabitation, during gestation, and until 21 days post parturition, and male rats for 60 days before cohabitation. No effects on mating or fertility were observed in rats up to 5 mg/kg/day which is approximately 100 times the MRHD of 0.5 mg/day, based on mg/m 2 body surface area.
HOW SUPPLIED/STORAGE AND HANDLING
Triazolam is supplied as a 0.125 mg white tablet or a 0.25 mg powder blue, scored tablet in the following strengths and package configurations:
| Package Configuration | Tablet Strength (mg) | NDC | |
|---|---|---|---|
Bottles of 10 | 0.125 mg | NDC 59762-3717-4 | G3717 |
Bottles of 100 | 0.125 mg | NDC 59762-3717-9 | G3717 |
Bottles of 10 | 0.25 mg | NDC 59762-3718-4 | G3718 |
Bottles of 100 | 0.25 mg | NDC 59762-3718-9 | G3718 |
Bottles of 500 | 0.25 mg | NDC 59762-3718-3 | G3718 |
Store at controlled room temperature 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature] .
Mechanism of Action
Triazolam is a benzodiazepine. Triazolam exerts its effect for the short-term treatment of insomnia through binding to the benzodiazepine site of the gamma-aminobutyric acid-A (GABA A ) receptors in the brain and enhances GABA-mediated synaptic inhibition.